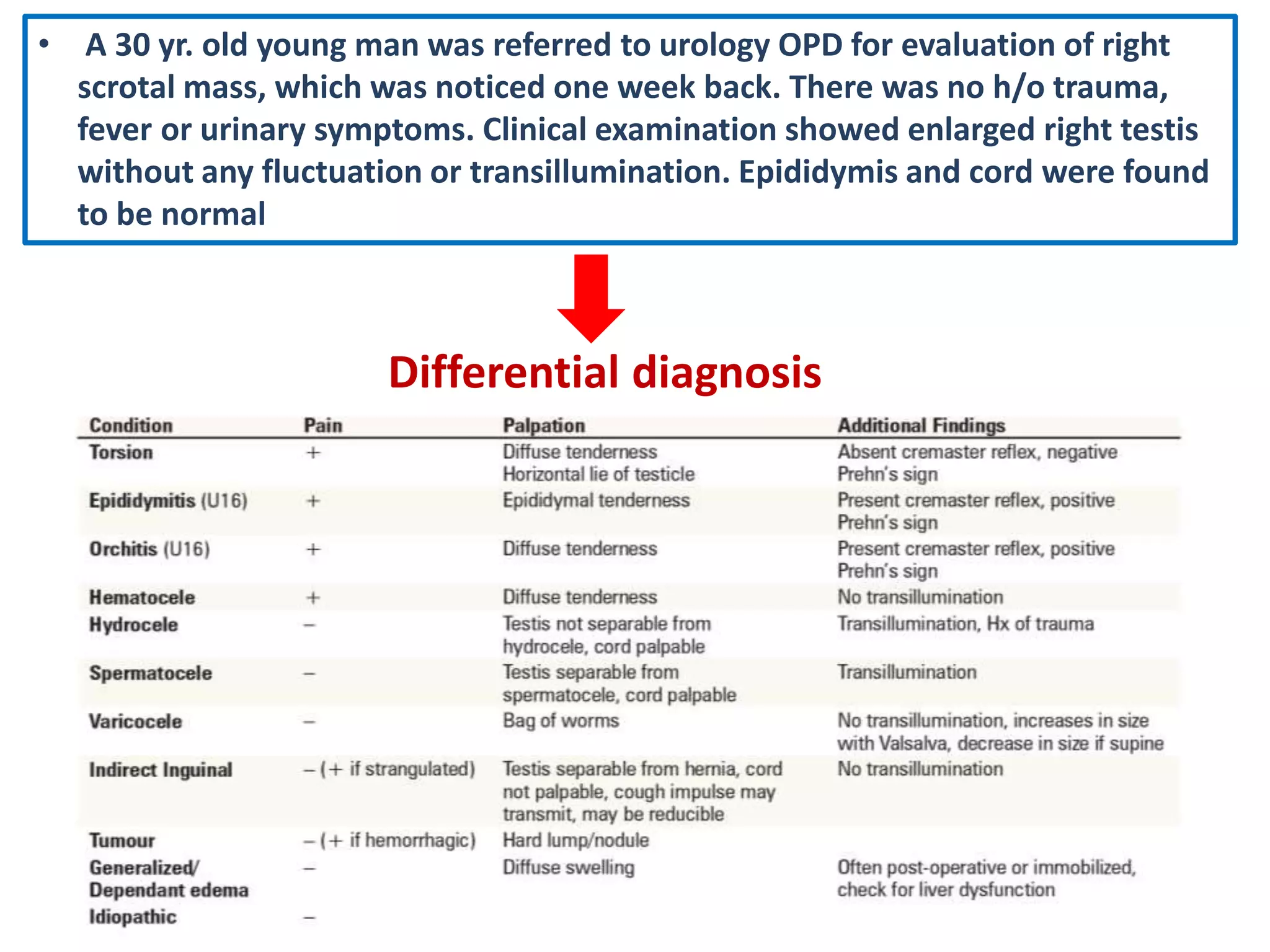
1) A 30-year-old man presented with right testicular swelling without pain or urinary symptoms. Examination found an enlarged right testis without tenderness or transillumination.
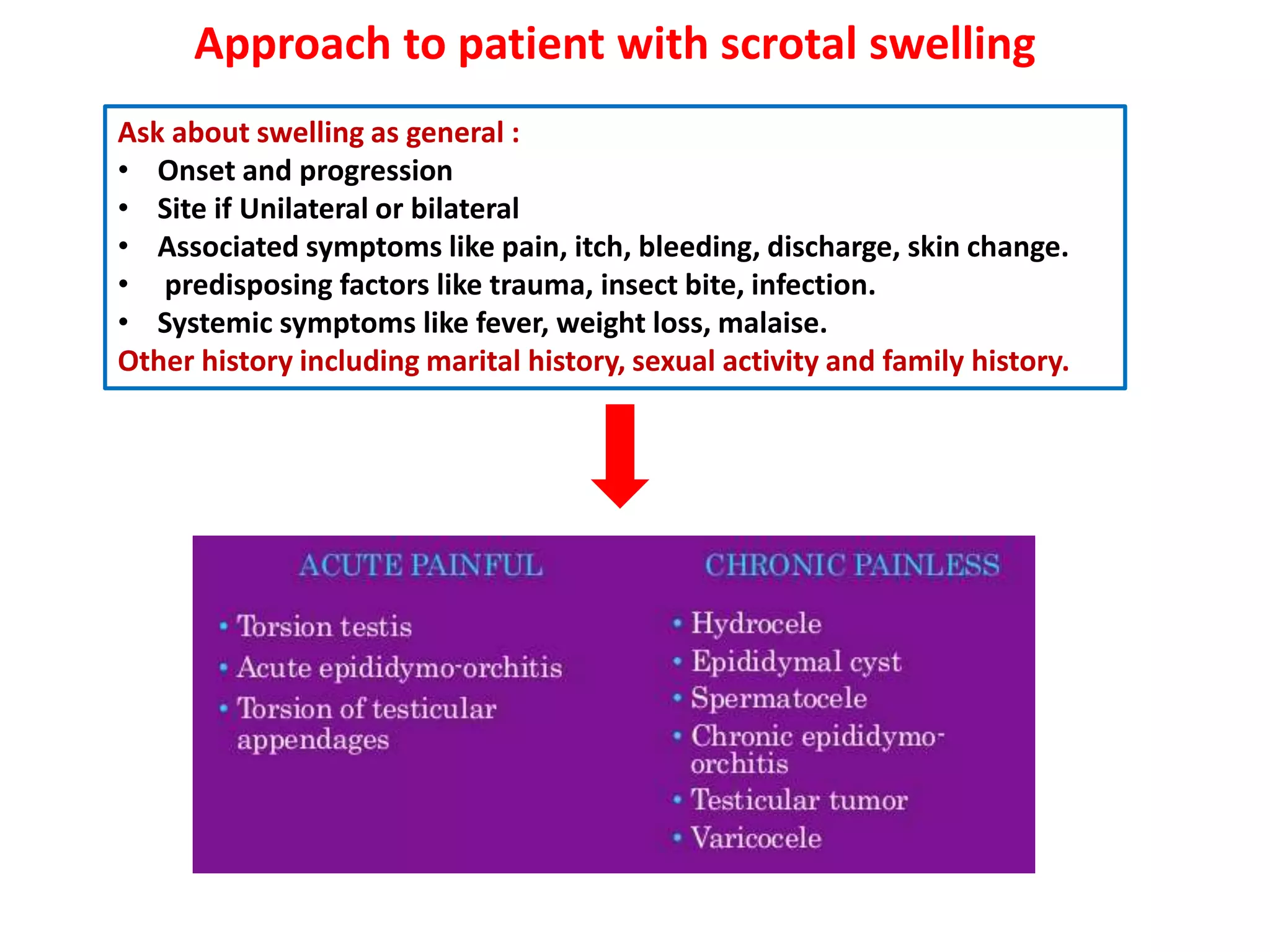
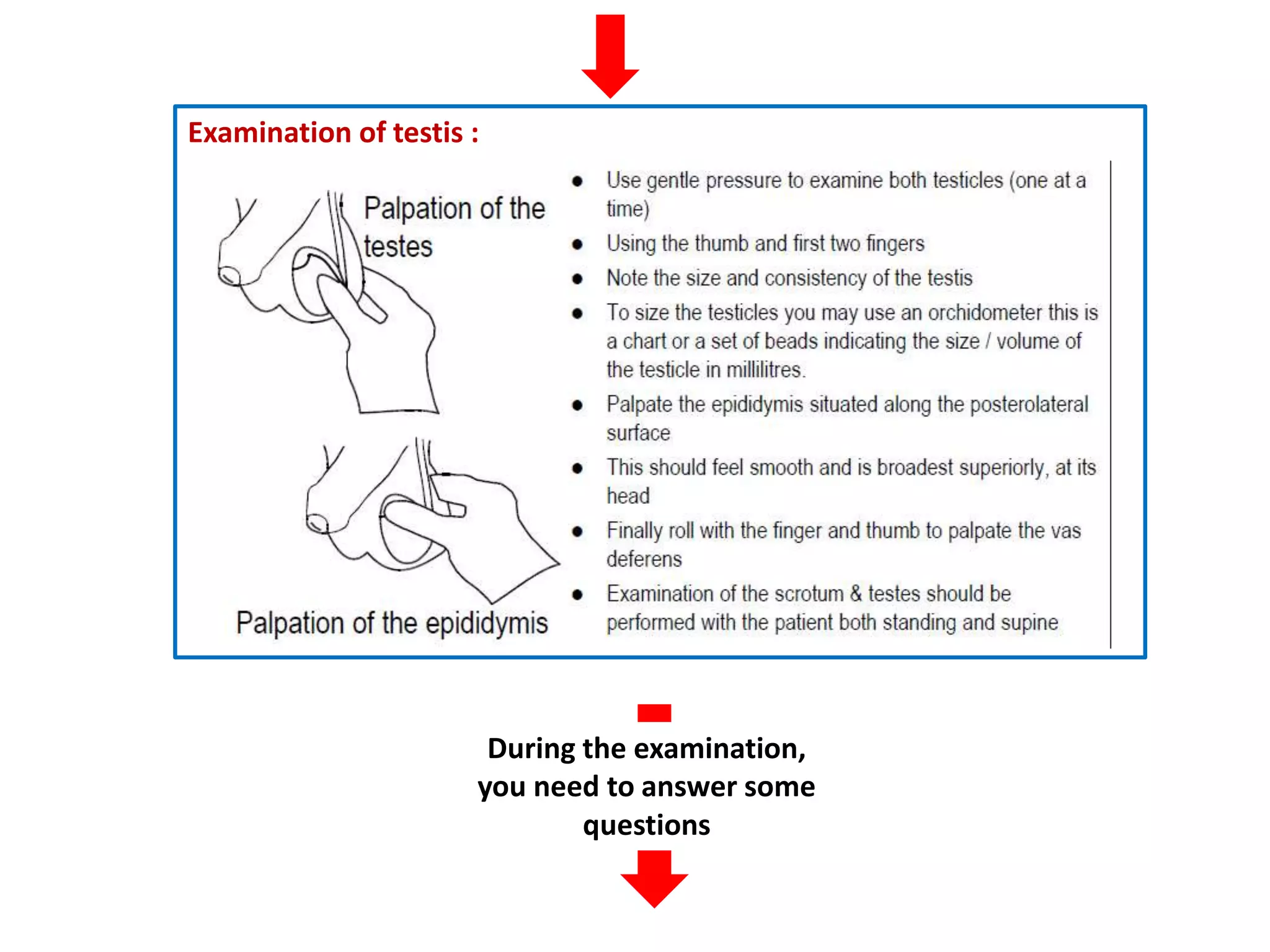
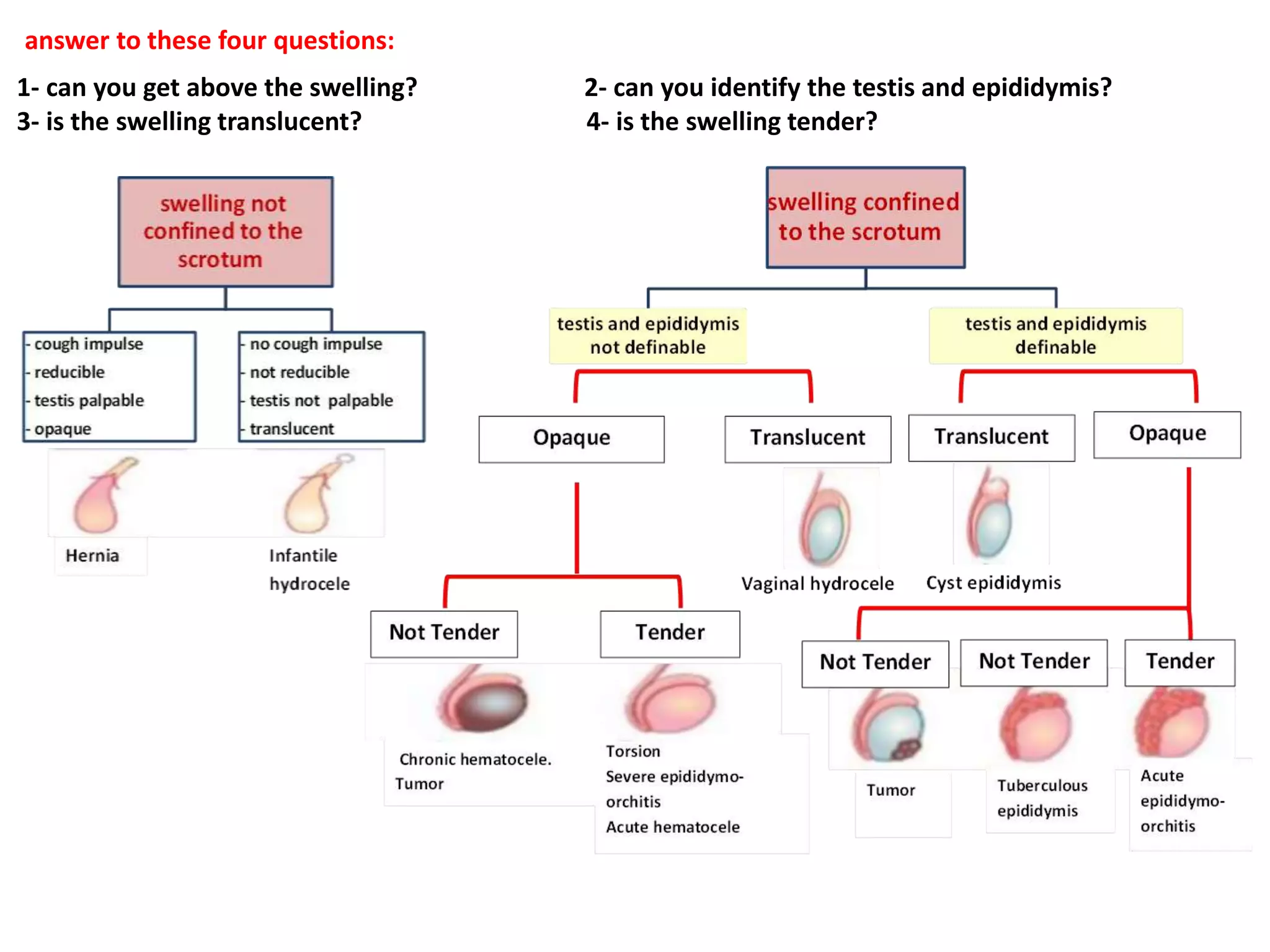
2) The document provides guidance on evaluating scrotal swellings, including asking about onset/progression, site, associated symptoms, and examination of the testis and epididymis.
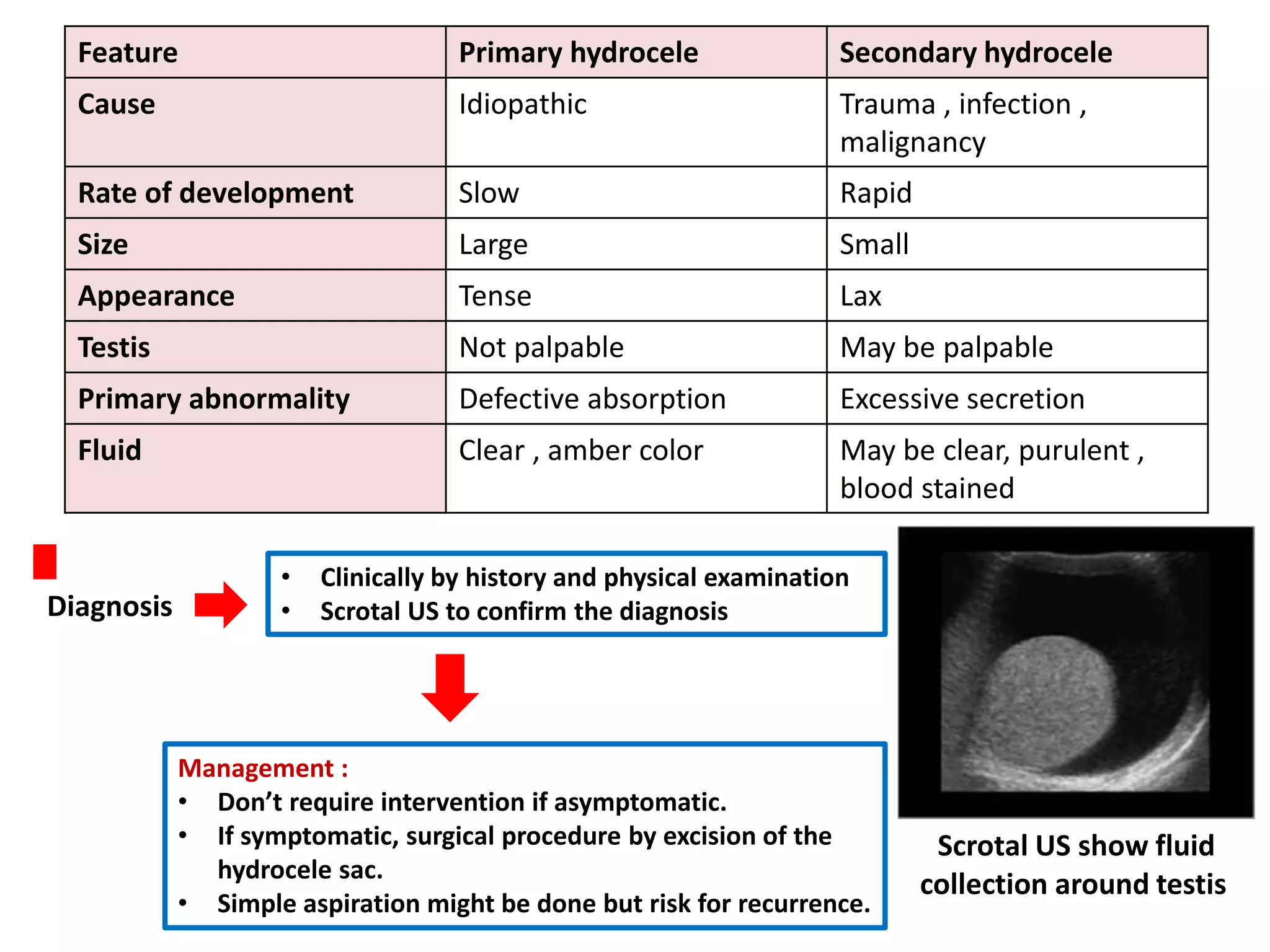
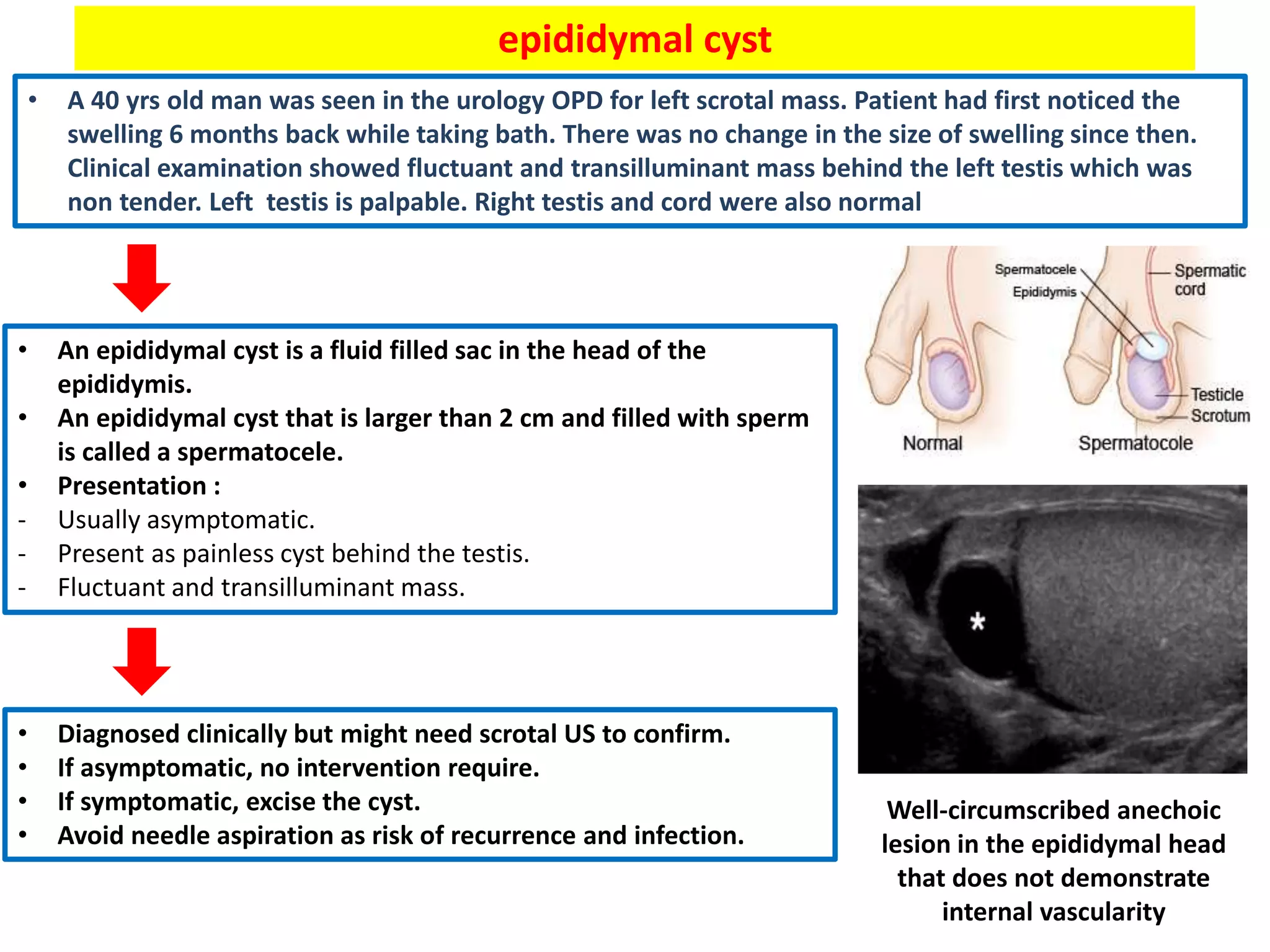
3) Common causes of scrotal swelling discussed are hydrocele, epididymal cyst, and varicocele. Hydrocele is fluid between the testis layers, epididymal cyst is a fluid sac in the epididymis, and varicocele is dilated spermatic veins.