Downloaded 312 times


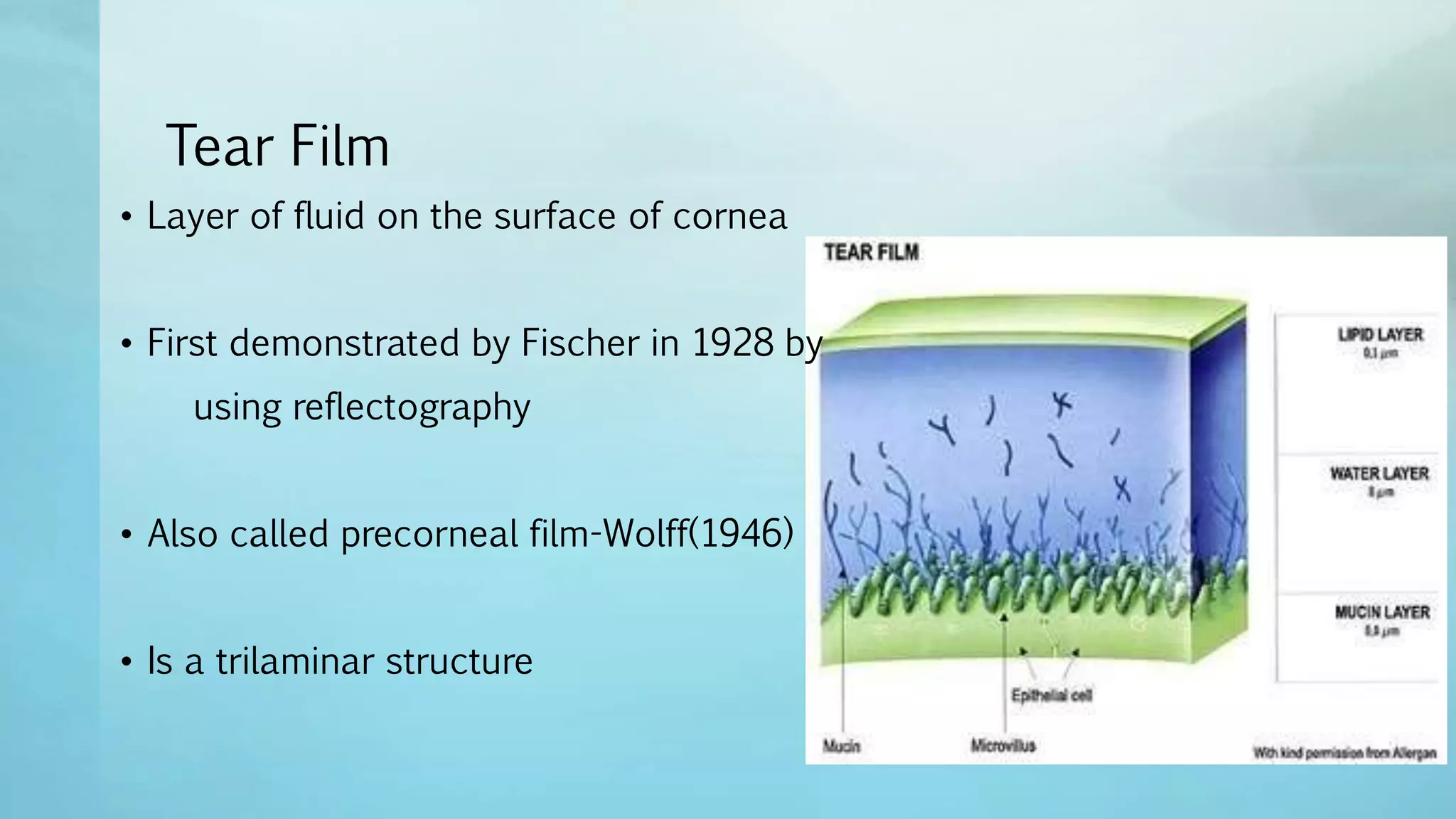























































































The document summarizes key aspects of the tear film and blinking. It describes the tear film as having three layers - an outer lipid layer, middle aqueous layer, and inner mucus layer. It discusses tear film composition, dimensions, dynamics of secretion, distribution, stability, flow, and drainage. Functions of the tear film include optical, protective, lubricative, osmotic, and nutritional roles. Blinking is described as the coordinated opening and closing of the eyelids, which aids tear secretion and distribution. Clinical tests for assessing tear quantity such as the Schirmer test and fluorescein clearance are also summarized.


































































![Presentation MOPA021 ANATOMY2 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/presentationmopa021anatomy2autosaved-230409101852-a55a7036-thumbnail.jpg?width=640&height=640&fit=bounds)




















