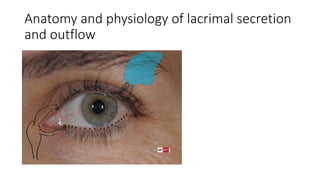
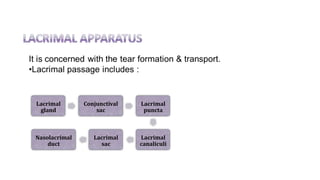
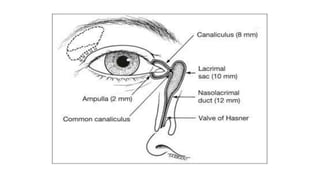
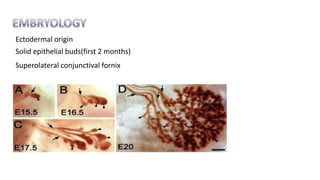
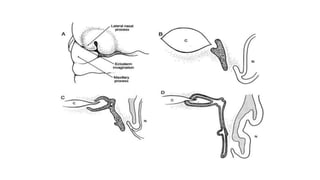
The document discusses the anatomy, development and physiology of the lacrimal secretory and drainage systems. It describes the embryological development of the lacrimal system from ectodermal tissue. It details the anatomy of the lacrimal gland, puncta, canaliculi, sac, duct and nasolacrimal drainage system. It explains the physiology of tear secretion, composition of the tear film layers, and the role of nerves, blood vessels and muscles in lacrimal secretion and drainage.