Download as PPSX, PPTX
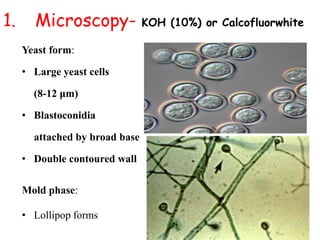
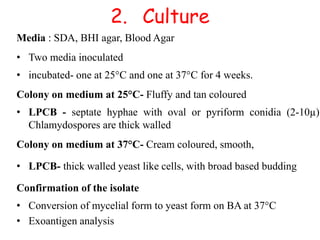

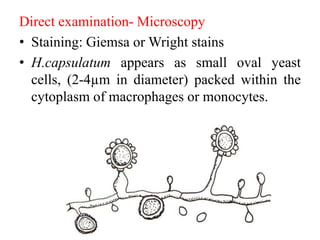


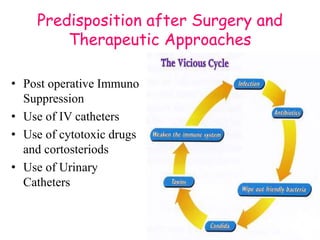
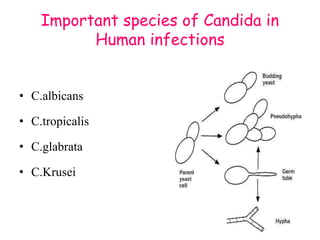
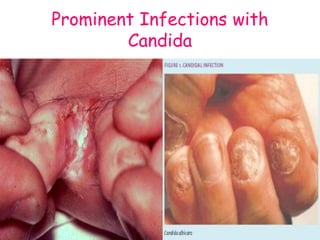
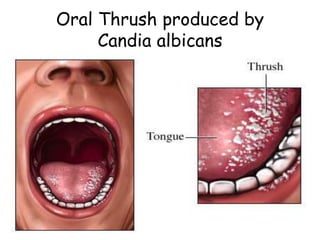
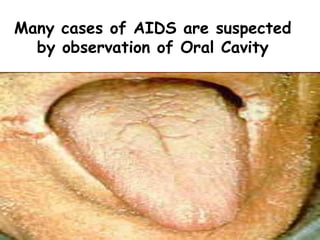
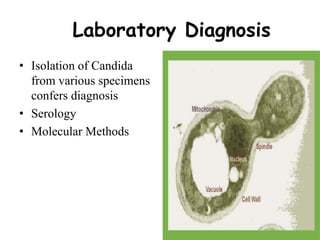
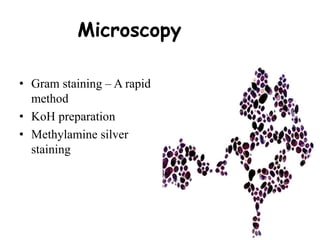
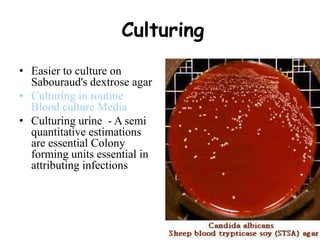
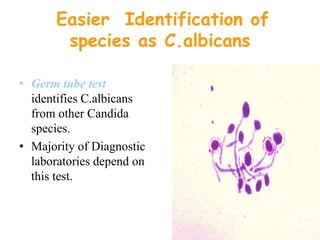
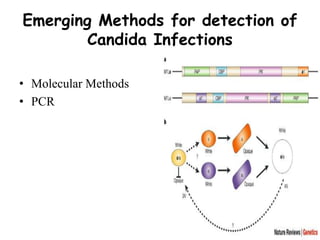
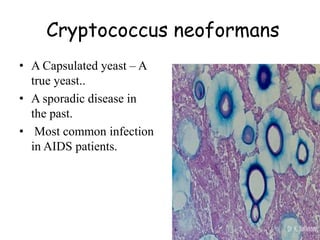


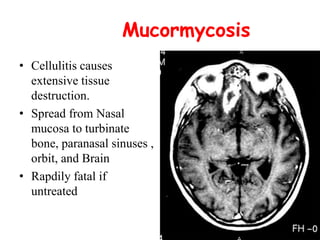
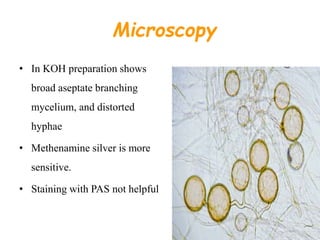
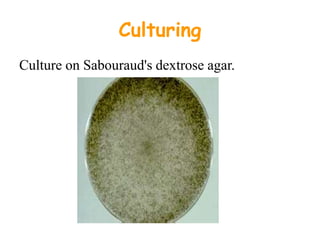


This document provides an overview of systemic and opportunistic mycoses. It defines systemic mycoses as deep fungal infections caused by soil-dwelling dimorphic fungi that are accidentally inhaled. The main causative agents described are Blastomyces dermatitidis, Paracoccidioides brasiliensis, Coccidioides immitis, and Histoplasma capsulatum. Opportunistic mycoses occur in immunocompromised individuals and the most common causes are Candida species, Aspergillus species, and Cryptococcus neoformans. Key clinical features, laboratory diagnostics including microscopy, culture, and serology, treatment approaches, and important epidemiological details are summarized

















































































