Downloaded 12 times

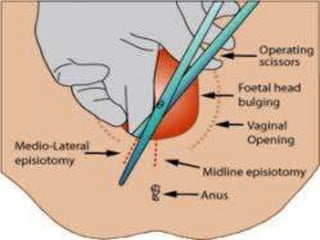
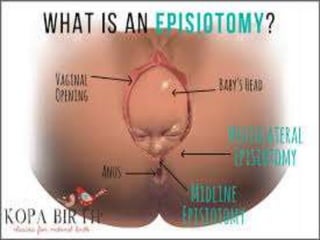





This document discusses episiotomy, which is a surgically planned incision made in the perineum and posterior vaginal wall during the second stage of labor. It aims to enlarge the vaginal opening to facilitate delivery and minimize tearing. Common indications include a rigid perineum, operative deliveries, or previous perineal surgery. The main types are mediolateral, median, and lateral incisions. A mediolateral episiotomy has advantages like less blood loss and easier repair compared to other types. The procedure involves preliminaries like anesthesia, followed by the incision and then repair of the vaginal mucosa, muscles, and skin in layers. Post-operative care and potential complications are also














































































