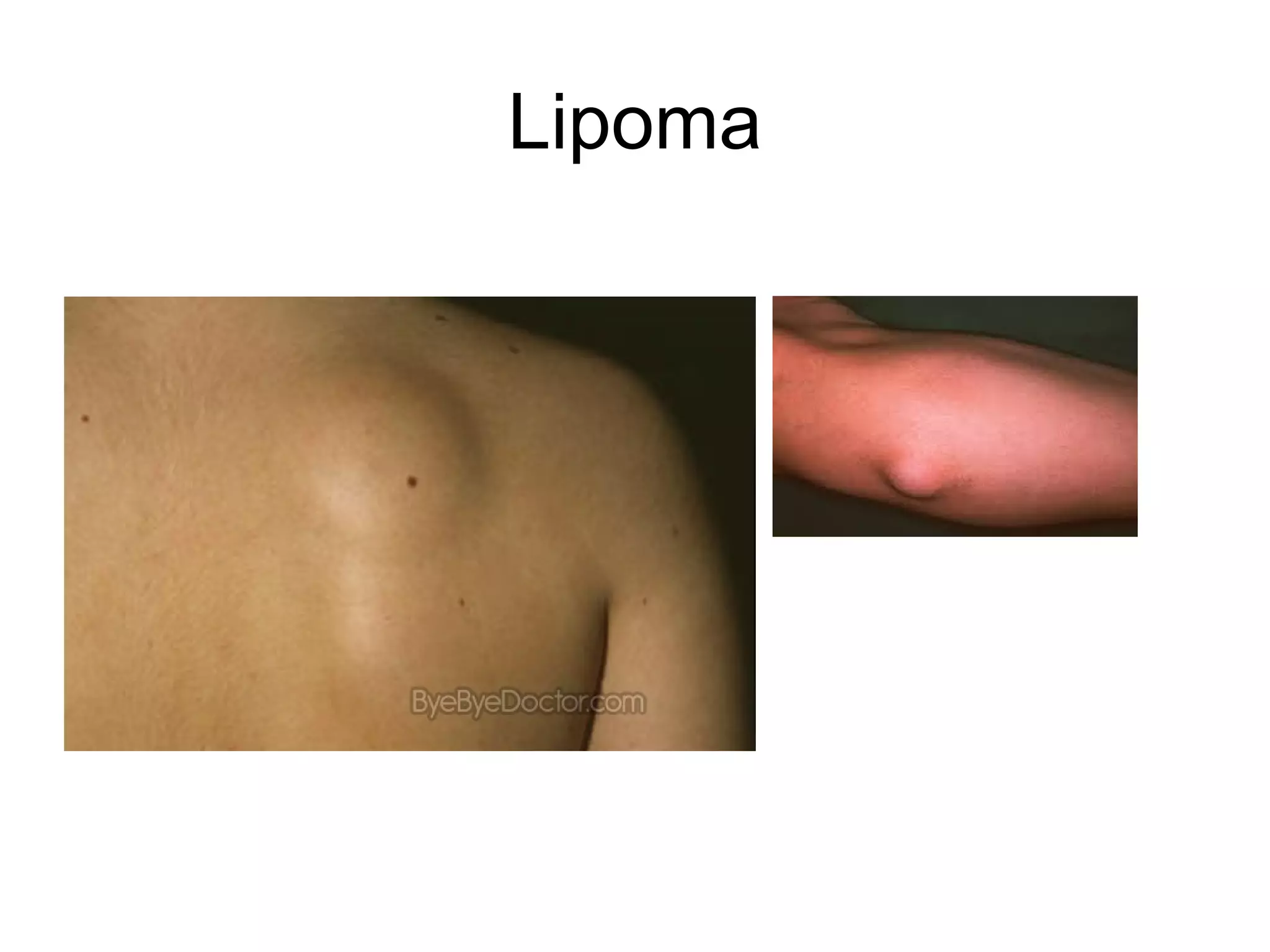
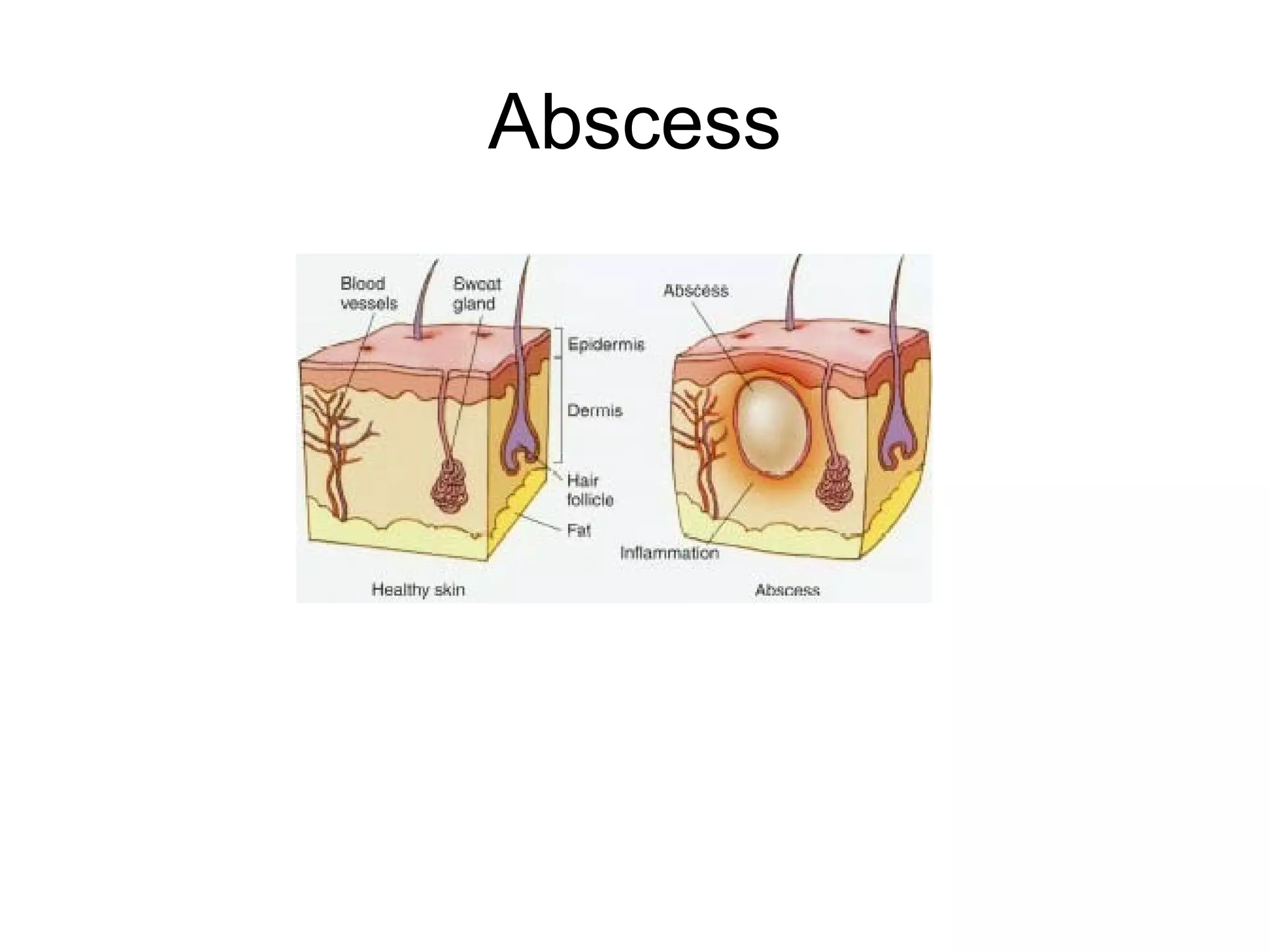
This document discusses soft tissue swellings like lipomas and sebaceous cysts. It focuses on abscesses, defining them as localized infections surrounded by inflamed tissue. Abscesses are commonly found on the extremities, buttocks, breast or perianal area. The document outlines indications for incision and drainage of abscesses, including those that are fluctuant or not resolving with antibiotics. It describes the materials, procedure, potential complications and follow up for incision and drainage of abscesses.