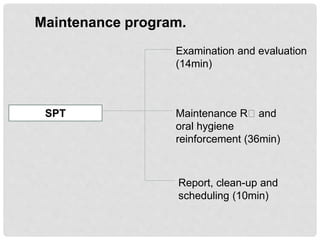
Supportive periodontal therapy (SPT) aims to prevent the recurrence and progression of periodontal disease in patients who have received prior treatment, with an emphasis on monitoring oral health and timely intervention for other oral diseases. The success of SPT relies significantly on patient compliance and understanding of their condition, as ongoing maintenance is crucial for prognosis. Regular examinations and evaluations are essential components of SPT, tailored to the patient's previous treatment and periodontal status.























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











