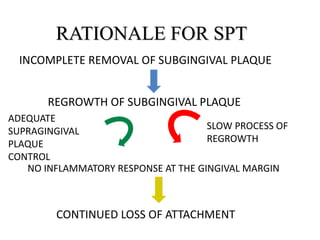
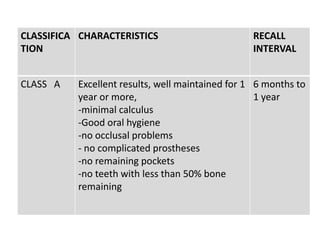
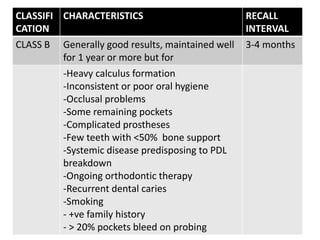
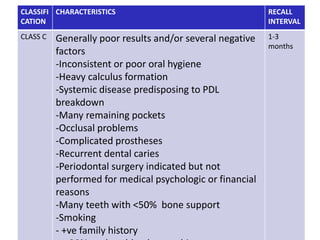
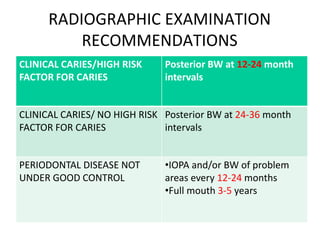
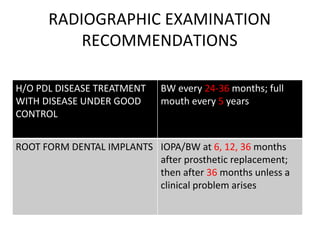
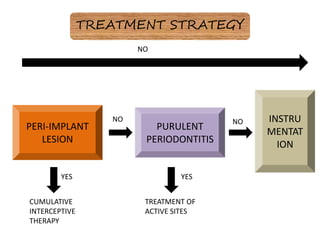
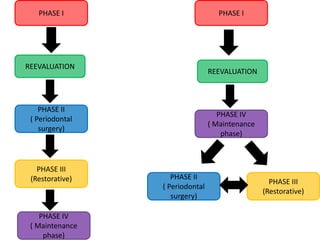
This document discusses supportive periodontal therapy (SPT), which involves maintenance care after initial treatment for periodontal disease. SPT is important for preventing recurrence of the disease and further tooth/bone loss. Long-term studies show that without SPT, periodontal disease often progresses again. The goals of SPT are to maintain periodontal health and reduce future tooth loss through regular cleanings and evaluation. Key aspects of SPT include subgingival plaque removal, risk assessment, and motivating patients to continue proper oral hygiene between visits. SPT has been shown to successfully maintain periodontal health for many years when done correctly.


![Loe et al [1978, 1986] conducted a longitudinal
investigation to study the natural development and
progression of periodontal disease.
The first study group established in Oslo,Norway
in 1969 ,consisted of 565 healthy male patients
between 17 to 40 years of age . Members of this group
experienced maximum exposure to conventional dental
care throught out their lives.](https://image.slidesharecdn.com/supportiveperiodontaltherapylast-230610153223-fd4dfbda/85/SUPPORTIVE-PERIODONTAL-THERAPY-last-ppt-32-320.jpg)