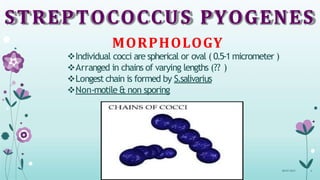
1) Streptococcus pyogenes is a gram positive bacterium that can cause a variety of infections in humans.
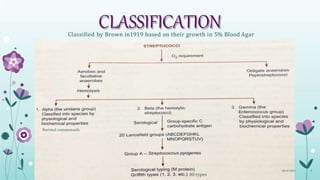
2) It is classified based on its hemolytic properties when cultured on blood agar as alpha, beta, or gamma hemolytic. S. pyogenes causes beta hemolysis.
3) S. pyogenes produces several toxins and enzymes that contribute to its virulence, allowing it to cause infections in the respiratory tract, skin, and other tissues. Common infections include pharyngitis, impetigo, cellulitis, and necrotizing fasciitis.





















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







