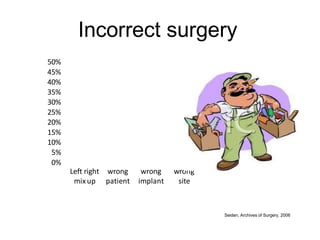
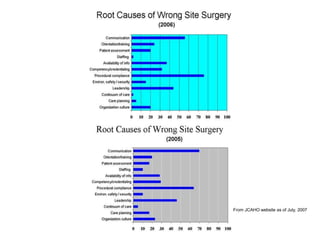
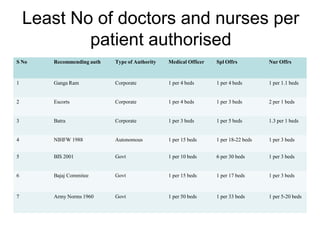
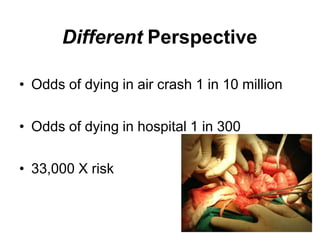
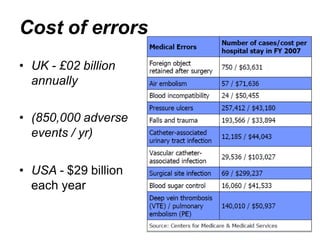
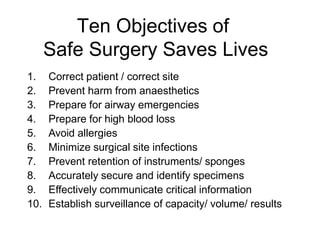
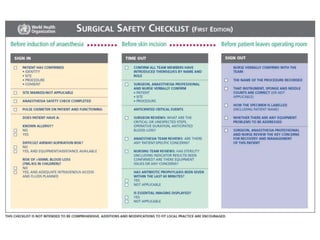
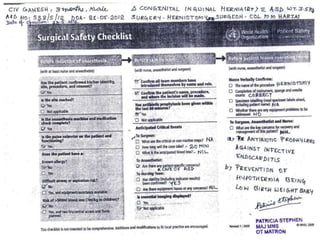
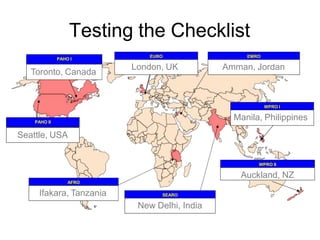
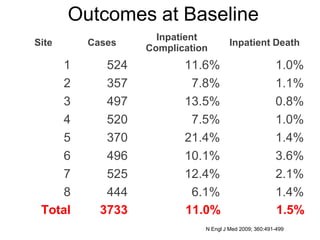
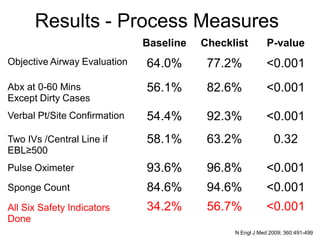
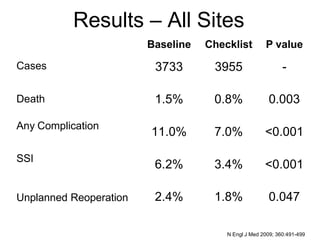
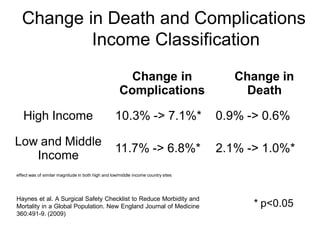
This document discusses surgical safety and errors. It notes that 234 million operations are performed globally each year, with 1 million deaths and 7 million disabling complications, over 50% of which are preventable. Common errors include wrong site surgery, wrong patient surgery, and retained surgical instruments. Causes of errors include lack of protocols, training, supervision, communication breakdowns, and operating outside of one's expertise. Checklists modeled after aviation safety checklists have been shown to reduce complications and deaths when used in surgery. A WHO surgical safety checklist was tested in 8 hospitals globally and significantly reduced death rates and complication rates. Universal adoption of checklists and a culture of safety are seen as keys to reducing preventable surgical errors.