Downloaded 226 times


![Stomach by kp [autosaved]](https://image.slidesharecdn.com/stomachbykpautosaved-140422141057-phpapp02/85/Stomach-by-kp-autosaved-55-320.jpg)

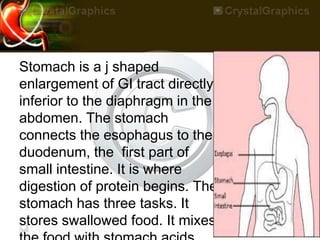
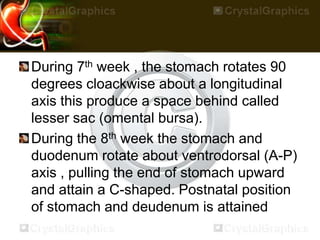
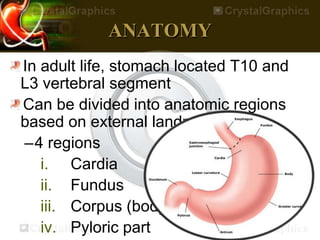
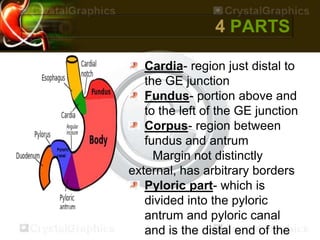
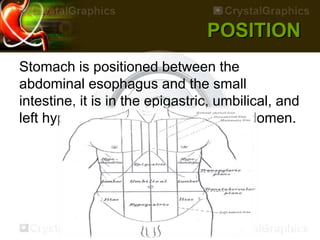
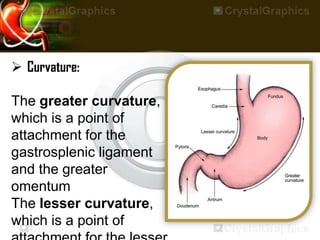
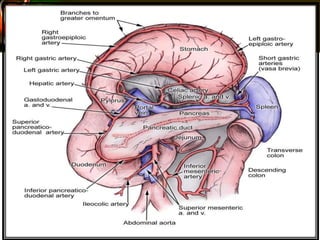
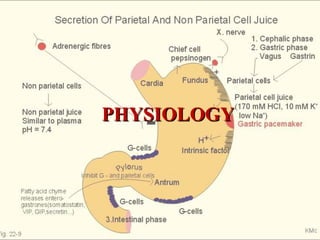
The stomach is a J-shaped organ located in the upper abdomen between the esophagus and small intestine. It has four regions - cardia, fundus, corpus, and pyloric part. The stomach stores and breaks down food through secretion of acids and enzymes. Motility mixes foods and empties contents into the small intestine. Diseases include peptic ulcers, gastritis, and stomach cancer.





























































![SURGICAL ANATOMY OF STOMACH [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/surgicalanatomyofstomachautosaved-230608035808-b982958c-thumbnail.jpg?width=640&height=640&fit=bounds)





















