General features
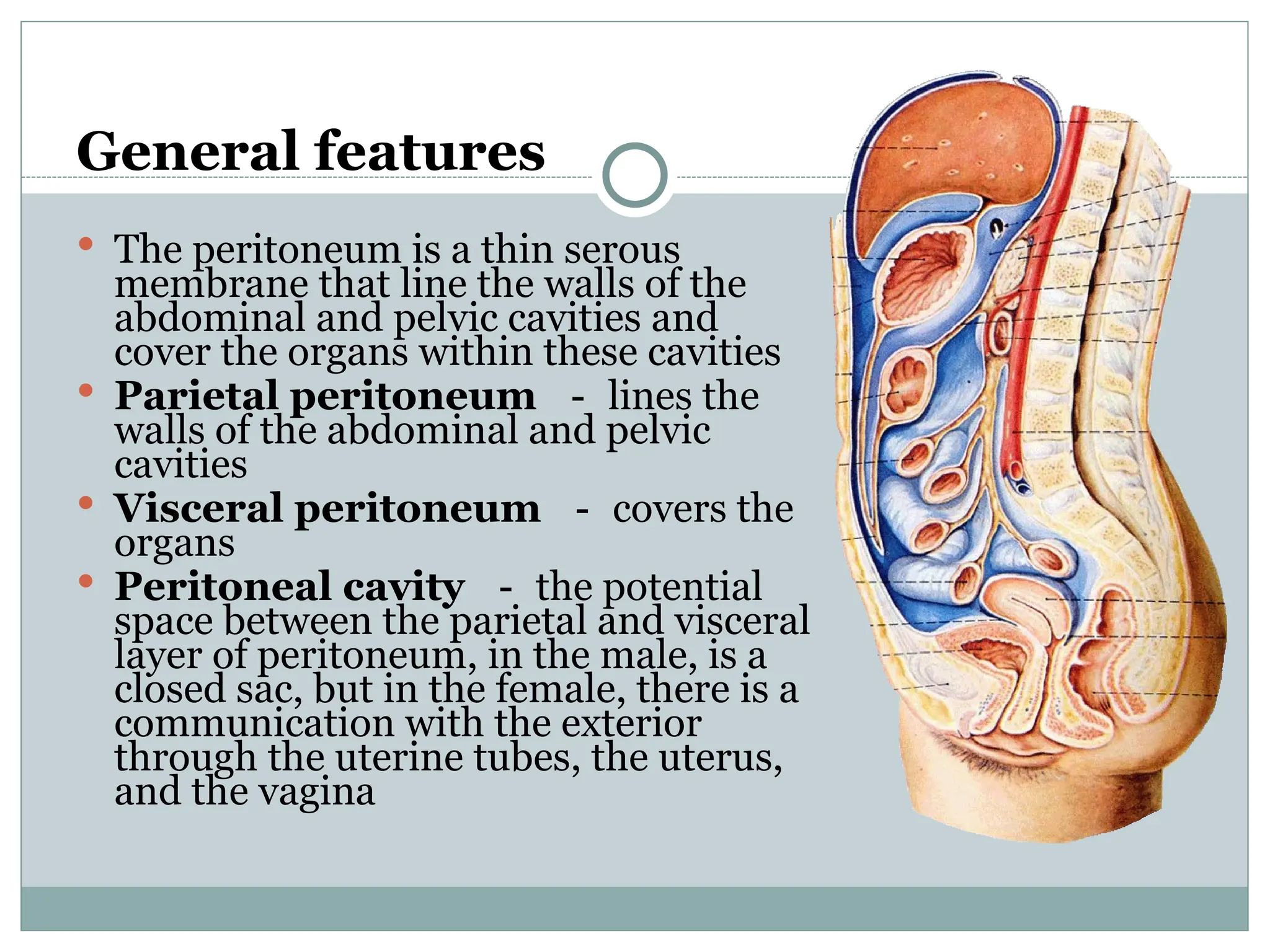
Theperitoneum is a thin serous
membrane that line the walls of the
abdominal and pelvic cavities and
cover the organs within these cavities
Parietal peritoneum - lines the
walls of the abdominal and pelvic
cavities
Visceral peritoneum - covers the
organs
Peritoneal cavity - the potential
space between the parietal and visceral
layer of peritoneum, in the male, is a
closed sac, but in the female, there is a
communication with the exterior
through the uterine tubes, the uterus,
and the vagina
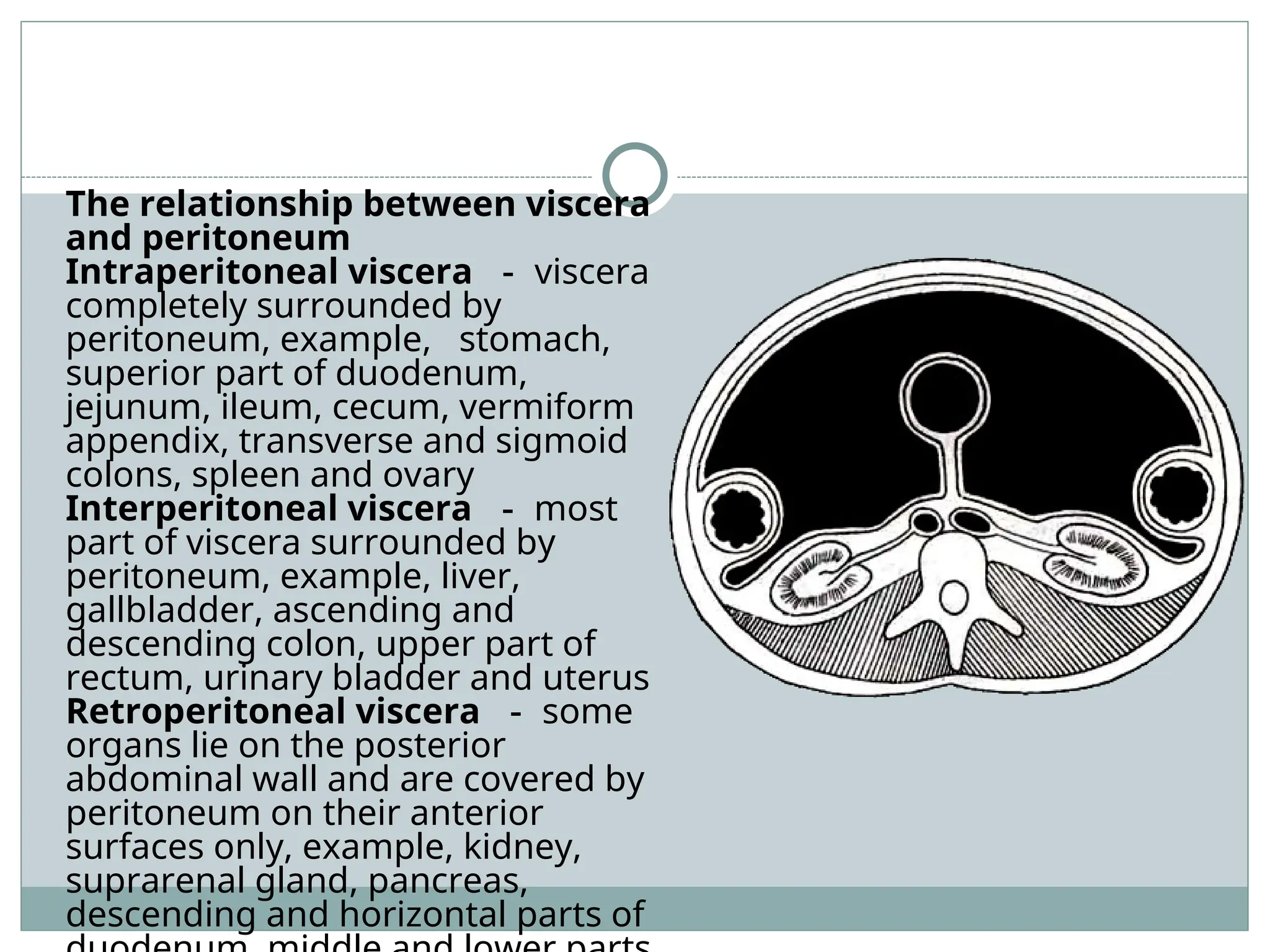
The relationship betweenviscera
and peritoneum
Intraperitoneal viscera - viscera
completely surrounded by
peritoneum, example, stomach,
superior part of duodenum,
jejunum, ileum, cecum, vermiform
appendix, transverse and sigmoid
colons, spleen and ovary
Interperitoneal viscera - most
part of viscera surrounded by
peritoneum, example, liver,
gallbladder, ascending and
descending colon, upper part of
rectum, urinary bladder and uterus
Retroperitoneal viscera - some
organs lie on the posterior
abdominal wall and are covered by
peritoneum on their anterior
surfaces only, example, kidney,
suprarenal gland, pancreas,
descending and horizontal parts of
6.
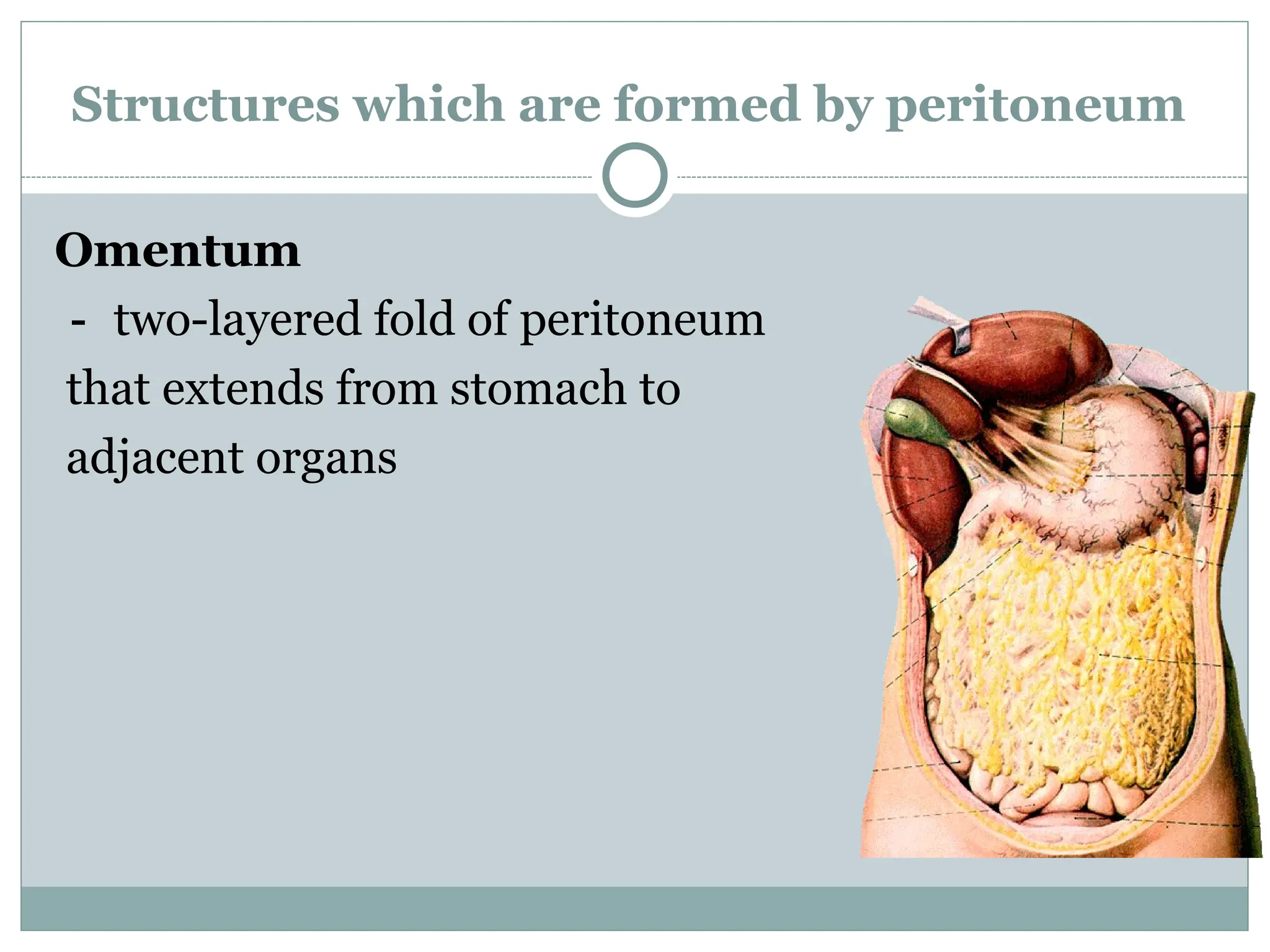
Structures which areformed by peritoneum
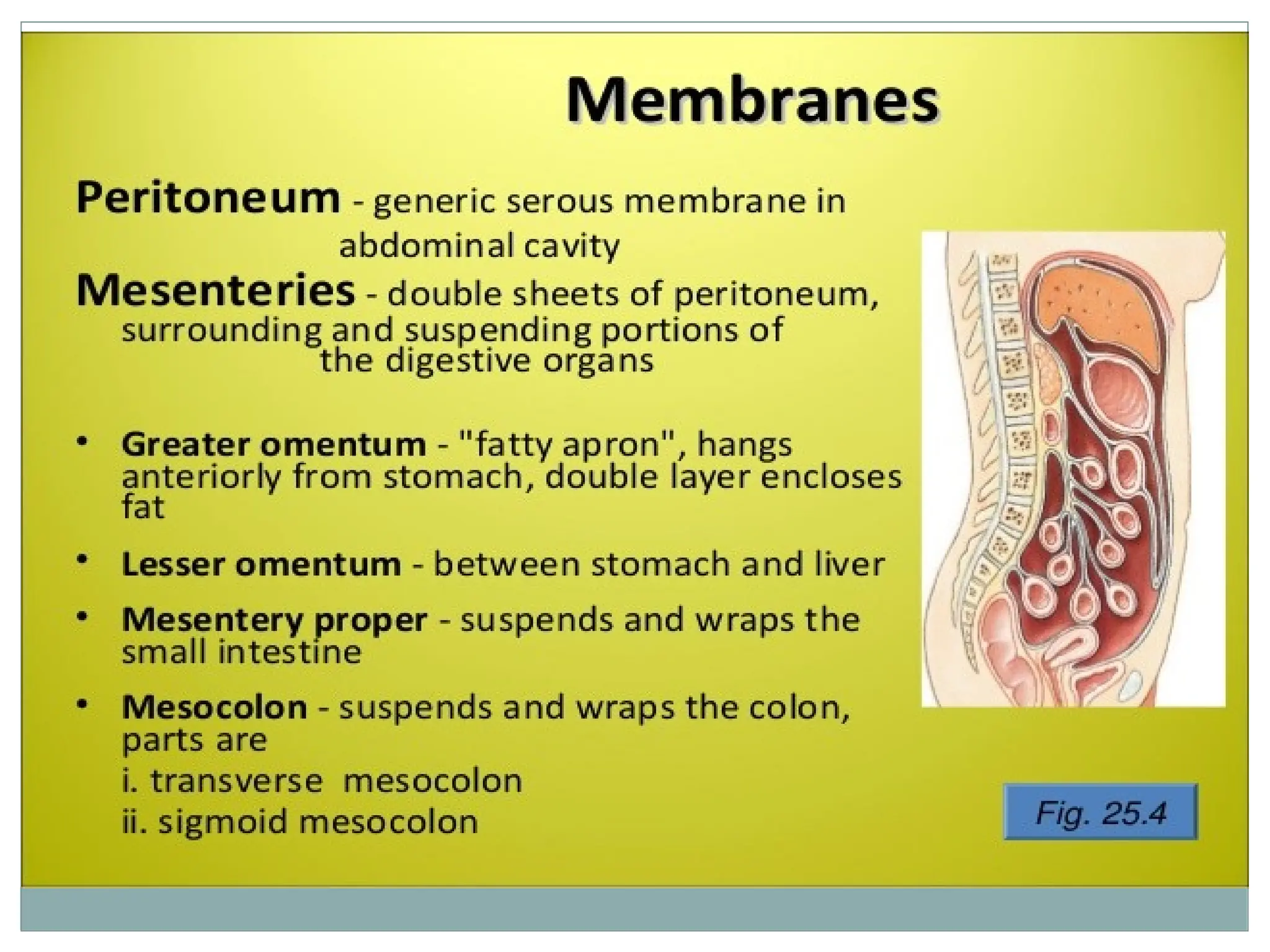
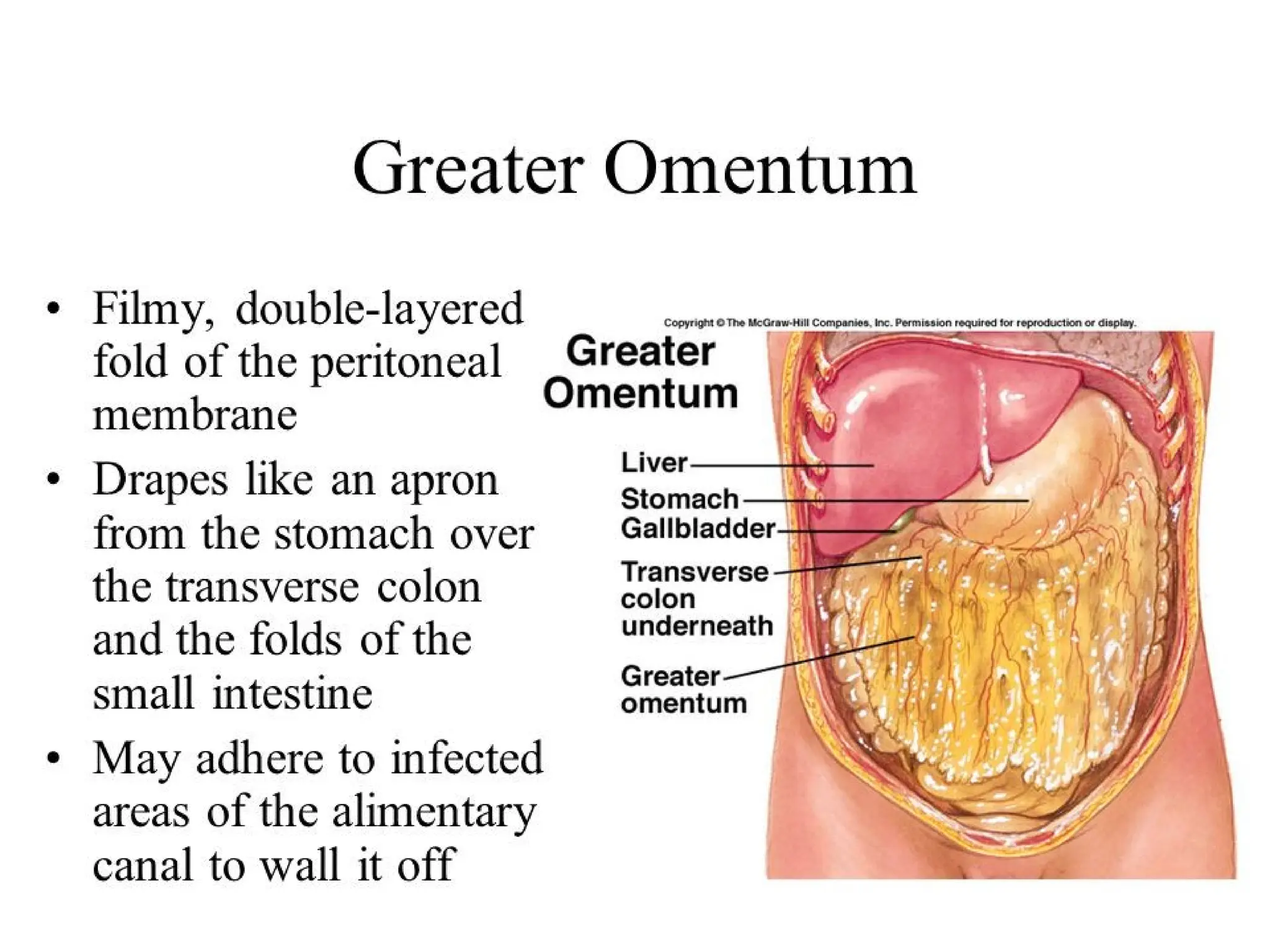
Omentum
- two-layered fold of peritoneum
that extends from stomach to
adjacent organs
7.
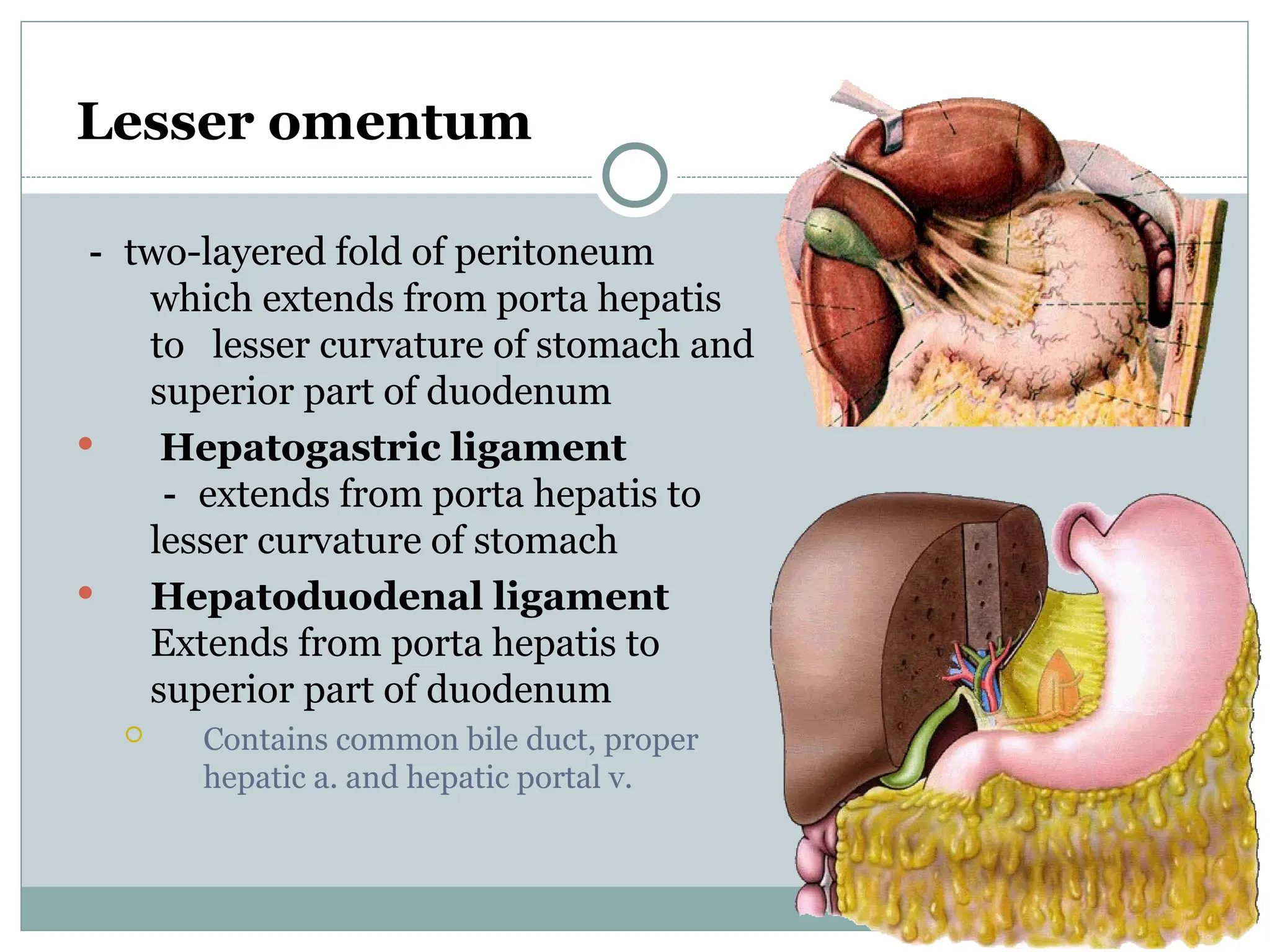
Lesser omentum
- two-layeredfold of peritoneum
which extends from porta hepatis
to lesser curvature of stomach and
superior part of duodenum
Hepatogastric ligament
- extends from porta hepatis to
lesser curvature of stomach
Hepatoduodenal ligament
Extends from porta hepatis to
superior part of duodenum
Contains common bile duct, proper
hepatic a. and hepatic portal v.
9.
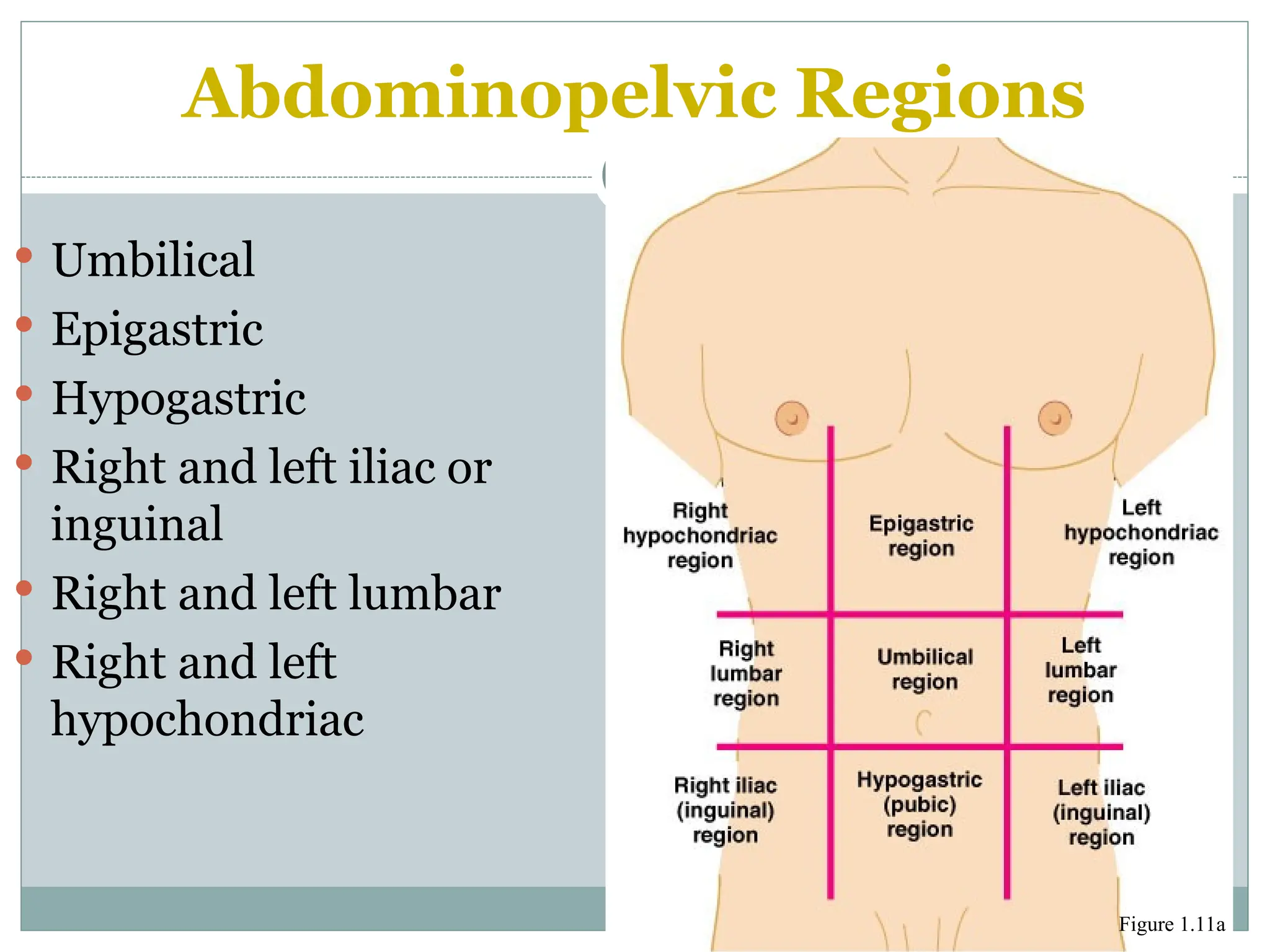
Abdominopelvic Regions
Umbilical
Epigastric
Hypogastric
Right and left iliac or
inguinal
Right and left lumbar
Right and left
hypochondriac
Figure 1.11a
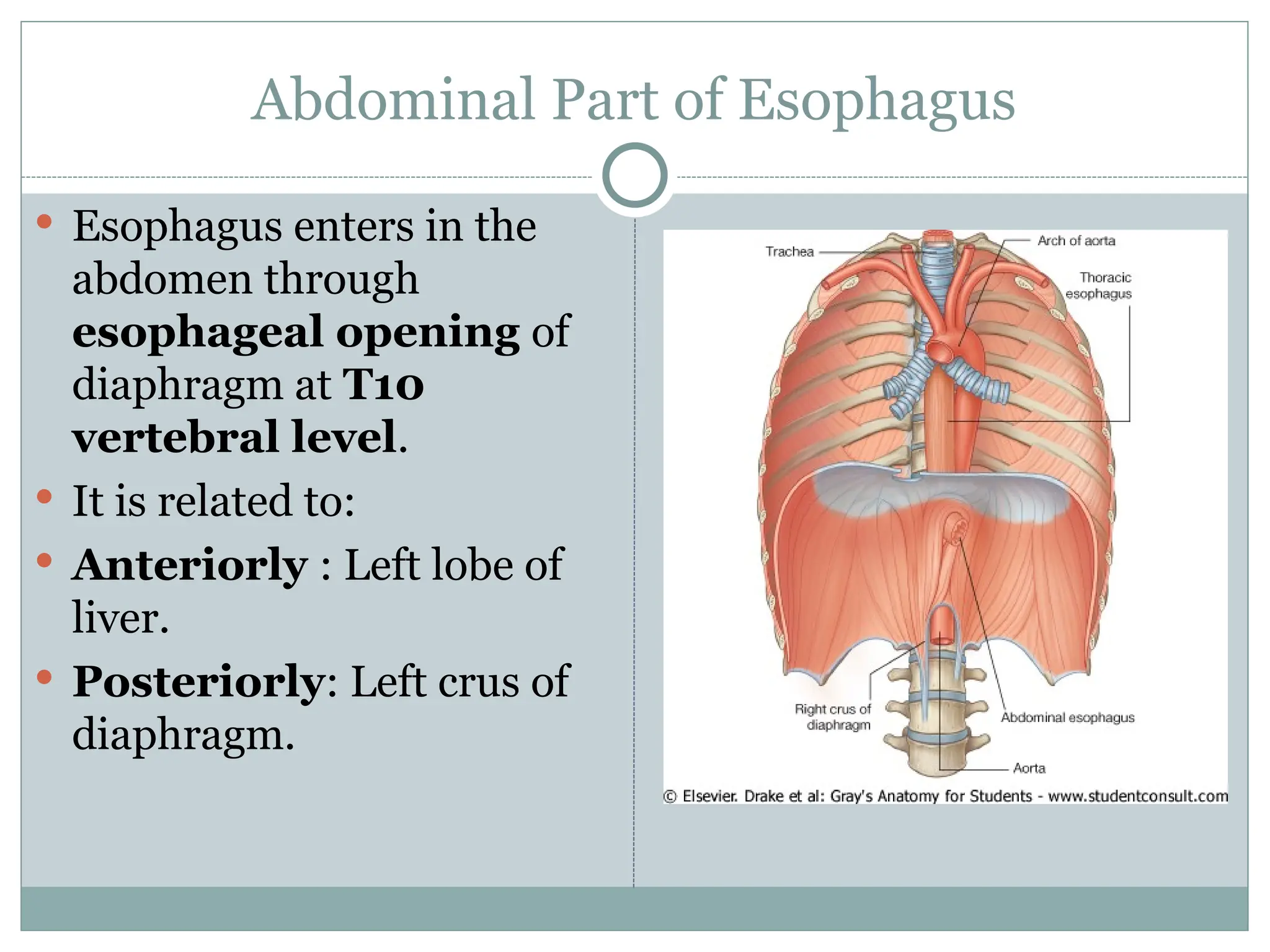
Abdominal Part ofEsophagus
Esophagus enters in the
abdomen through
esophageal opening of
diaphragm at T10
vertebral level.
It is related to:
Anteriorly : Left lobe of
liver.
Posteriorly: Left crus of
diaphragm.
14.
Blood supply andNerve supply of Abdominal
Part of Esophagus
Blood supply:
Arterial supply: Left
gastric artery from
Coeliac trunk.
Venous drainage: Left
gastric vein tributary of
Portal vein
Lymphatic drainage: Left
gastric and coeliac lymph
nodes
Nerve Supply:
Parasympathetic: Vagus
nerves
Sympathetic: Thoracic
sympathetic chain
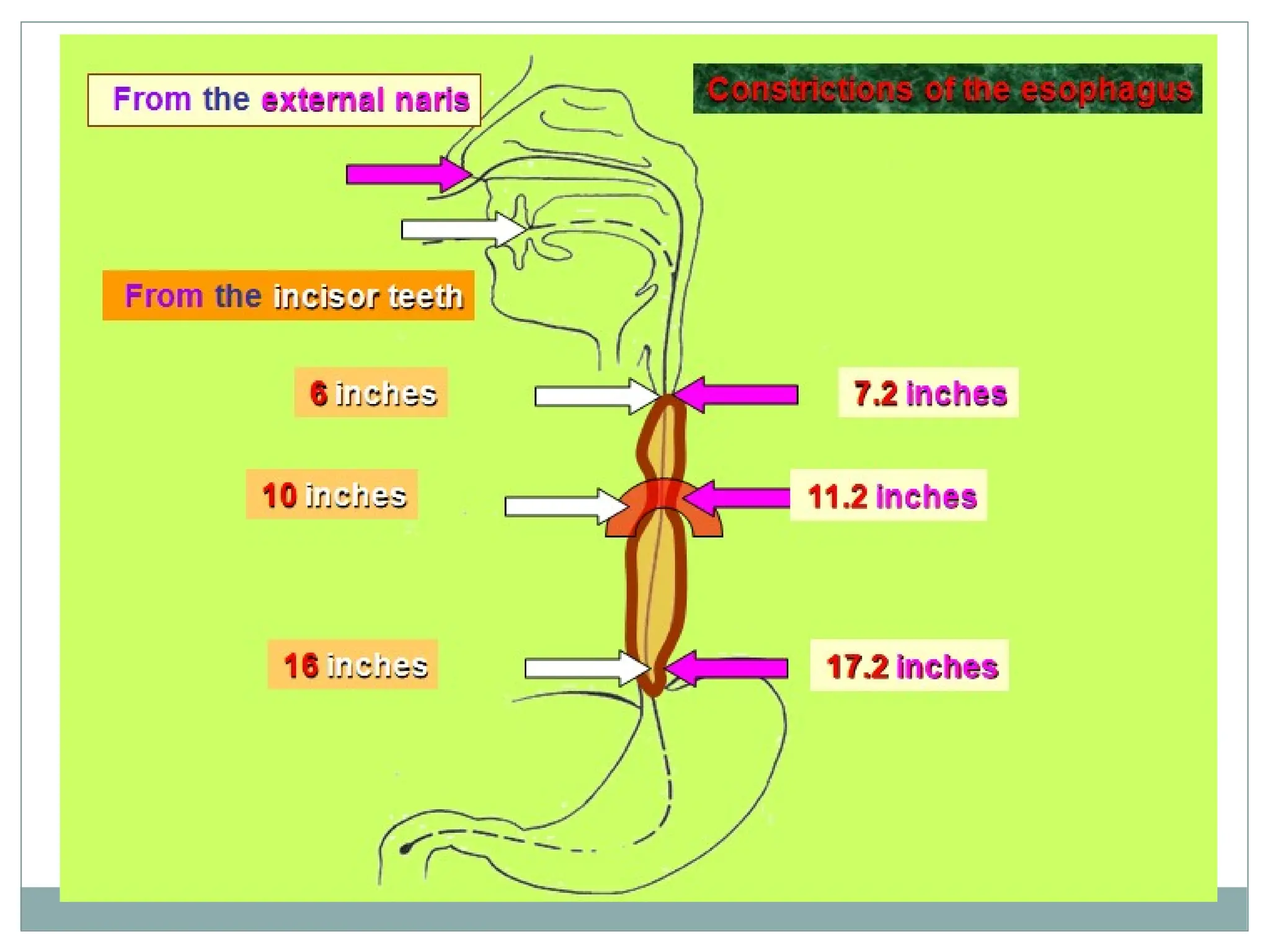
Esophageal Constrictions
Esophagushas three constrictions:
1. At its upper end, where it joins the Pharynx.
2.Near its middle, where it is crossed by the arch of
aorta and left main bronchus.
3.Near its lower end, where it pierces the diaphragm.
The approximate distances:
From the incisor teeth to these constrictions are 6,10 and 16
inches ( 15, 25 and 41 cms) respectively.
From the external nares to these constrictions are 7.2, 11.2
and 17.2 inches ( 18, 28 and 44 cms) respectively.
18.
Porto-systemic Venous Anastomosis
The lower end of the esophagus is an important site
of Porto-systemic anastomosis between the
esophageal tributaries of the Azygos vein (Systemic)
and the left gastric vein (Portal).
Importance:
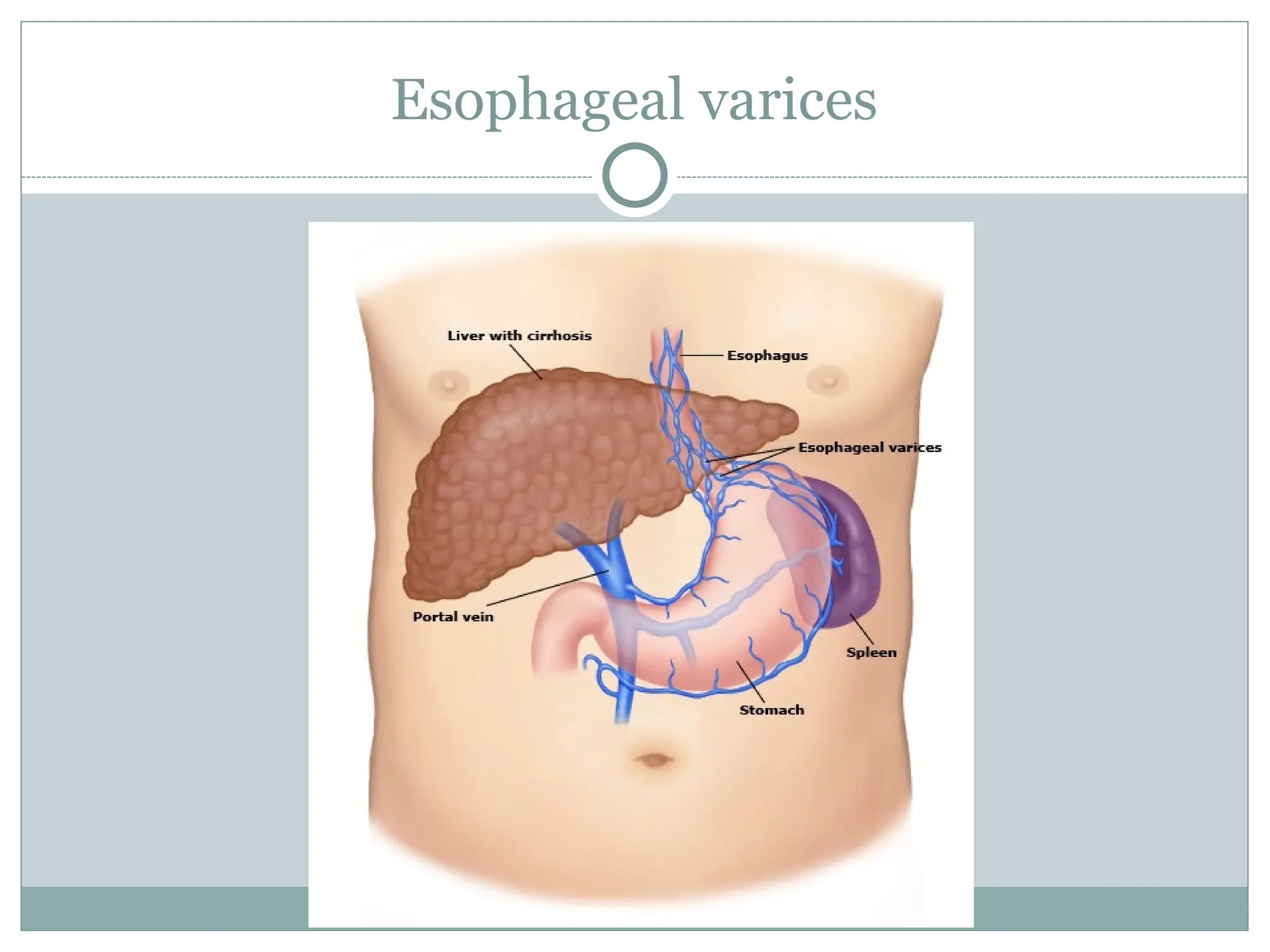
In case of postal obstruction in cirrhosis of liver,
Portal hypertension occurs. It results in dilatation of
this anastomosis and forms esophageal varices.
These varicose veins (varices) may rupture and cause
severe bleeding in the stomach and vomiting of blood
known as Hematemesis.
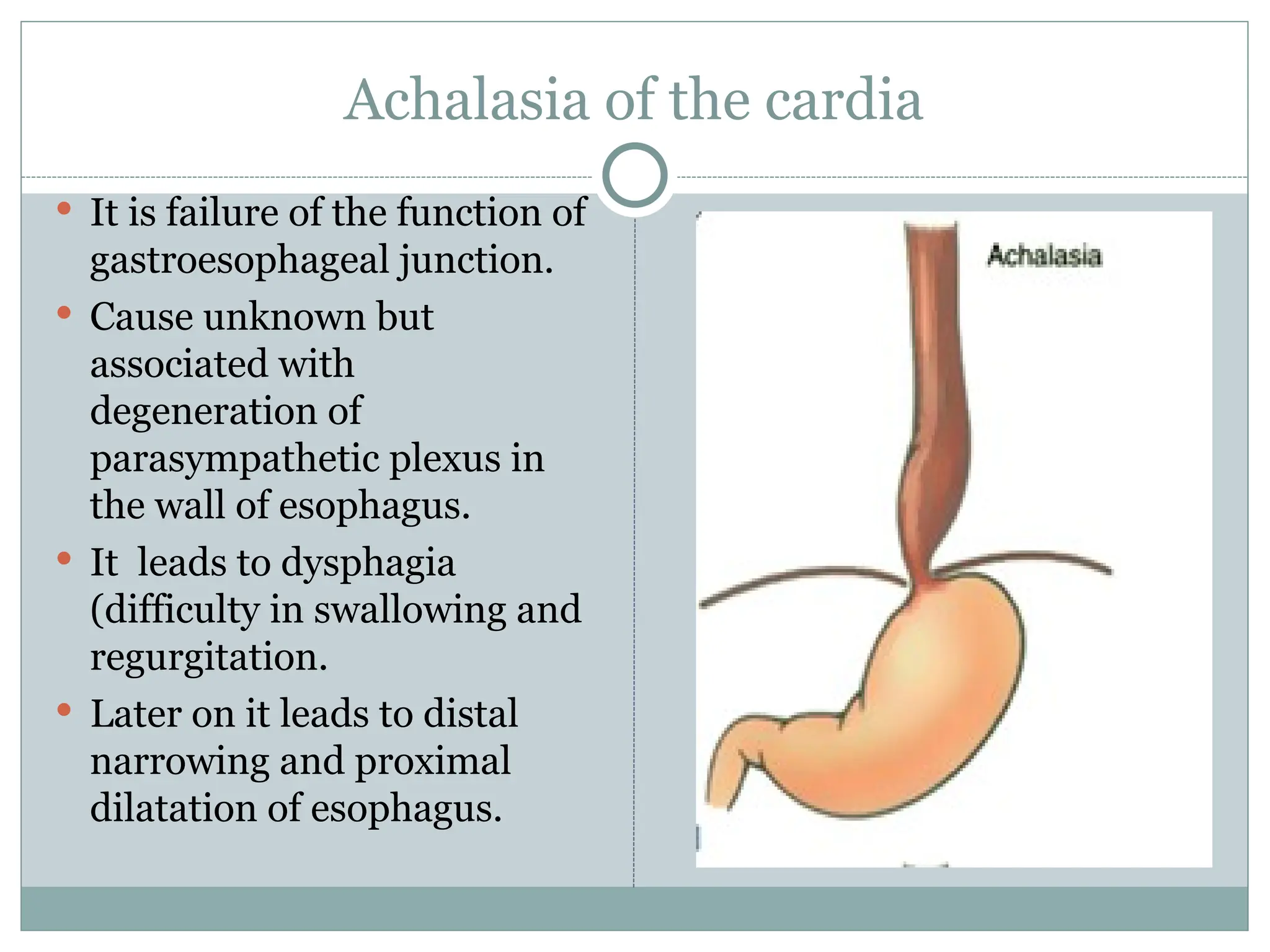
Achalasia of thecardia
It is failure of the function of
gastroesophageal junction.
Cause unknown but
associated with
degeneration of
parasympathetic plexus in
the wall of esophagus.
It leads to dysphagia
(difficulty in swallowing and
regurgitation.
Later on it leads to distal
narrowing and proximal
dilatation of esophagus.
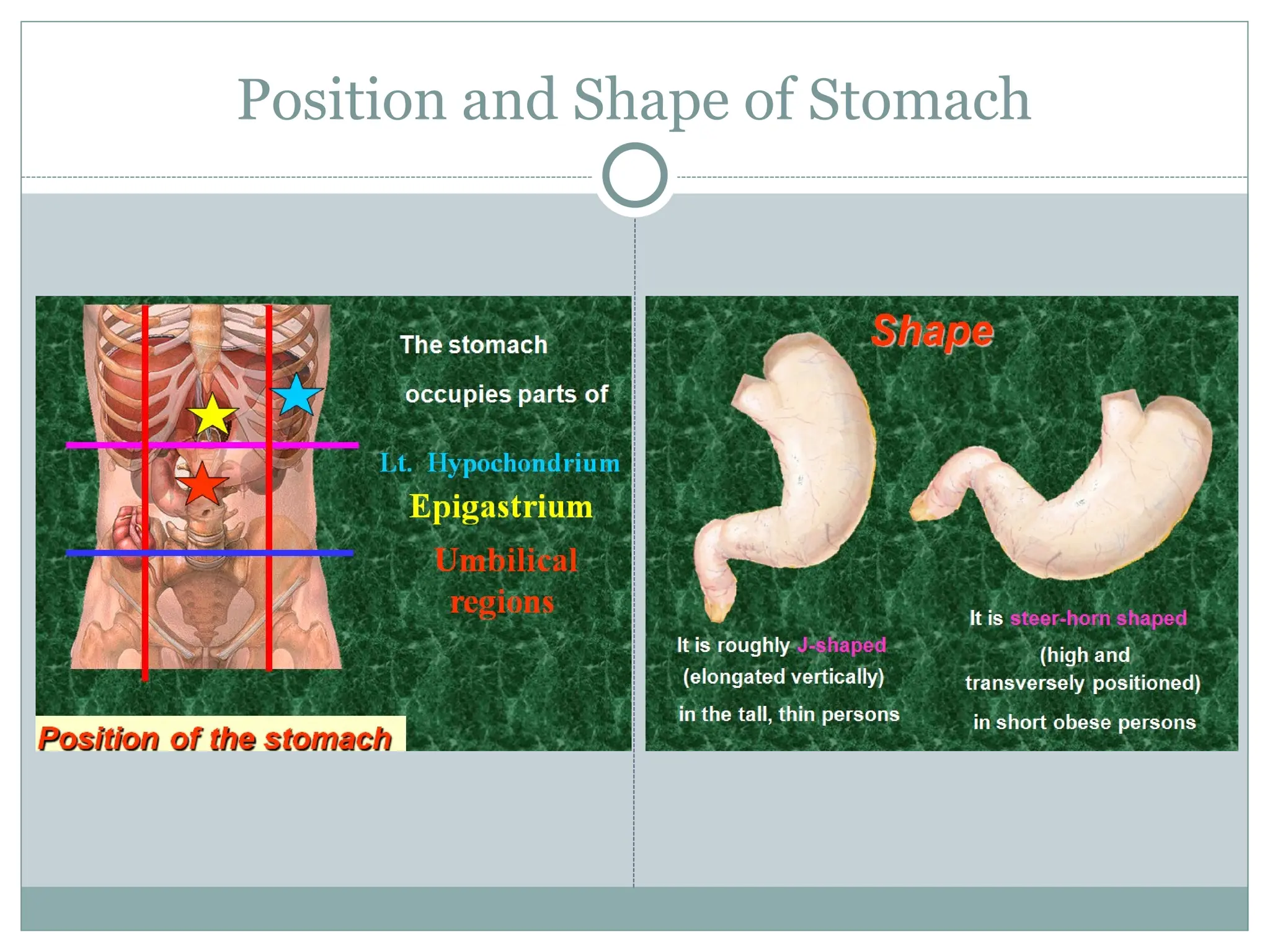
Position and Shape
Stomach is dilated part of GIT responsible for
storage and mixing of food.
Position: Occupy Left hypochondrium, epigastrium
and umbilical regions.
Shape:
In tall and thin persons: J-Shaped (Elongated
vertically.
In short obese persons: Steer-horn shape (High and
transversely placed)
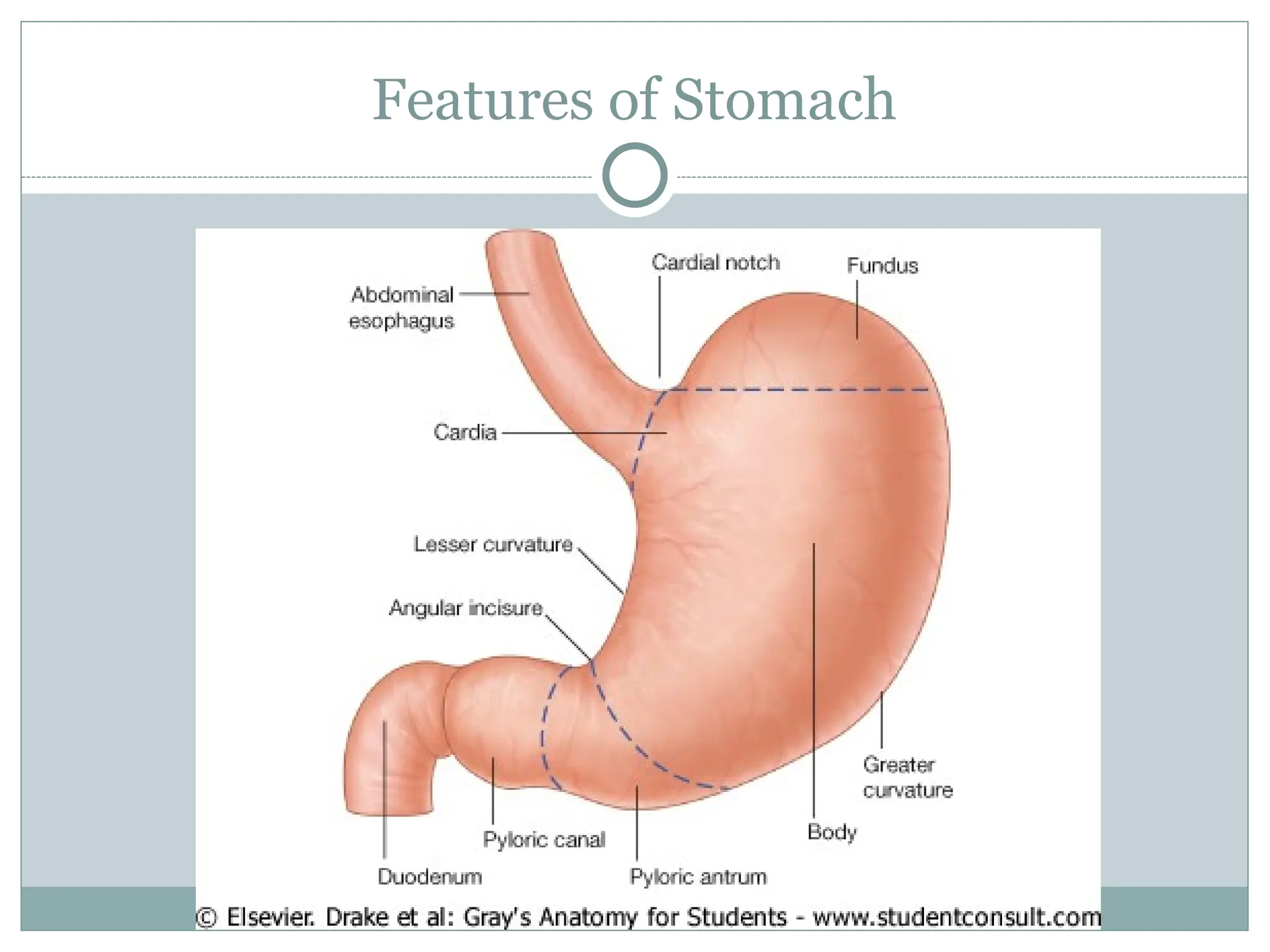
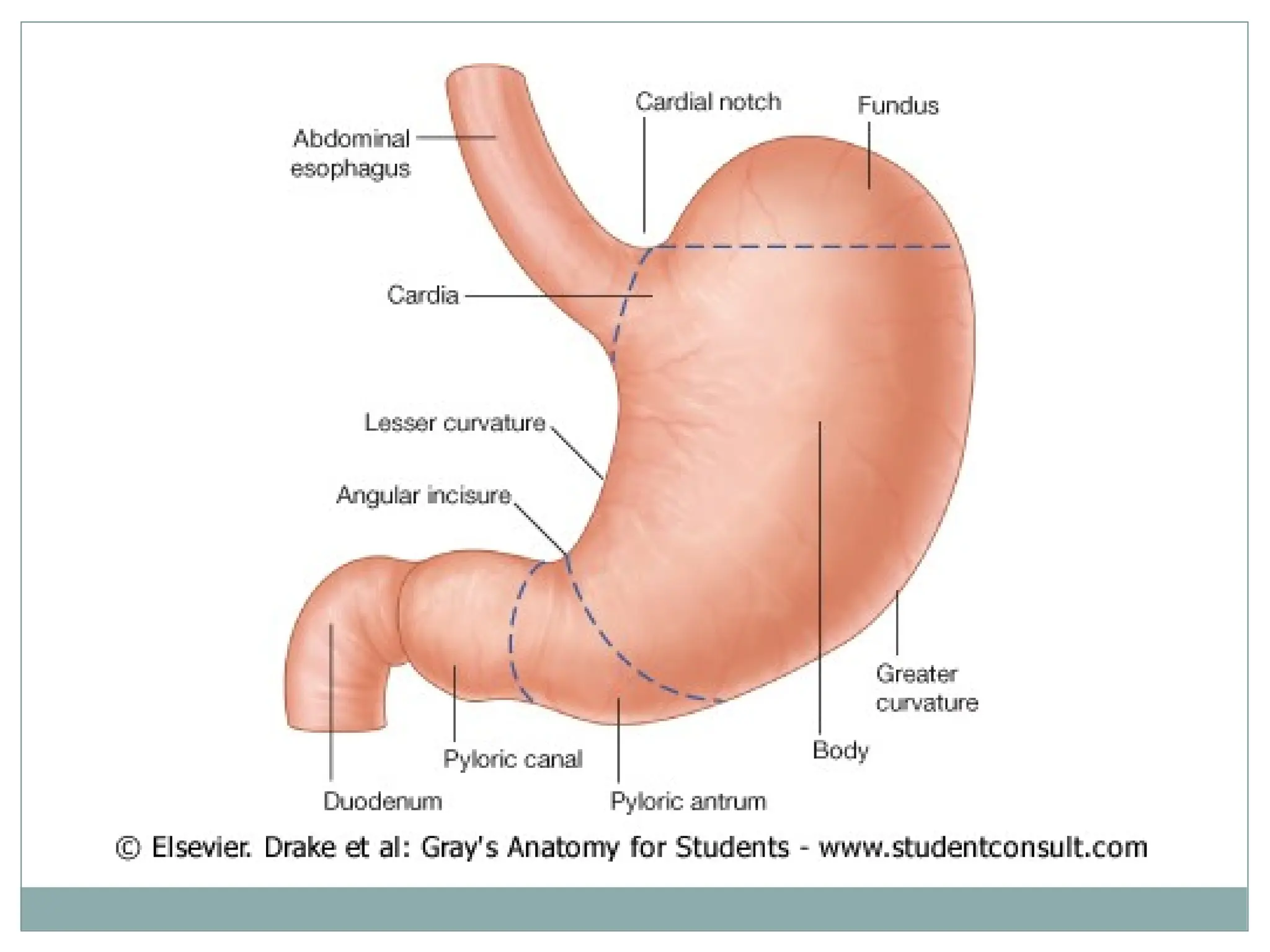
Features of stomach
Ends (Openings):
Cardiac End (Opening): Upper end at the junction with the
esophagus.
Pyloric End (Opening): Lower end at the junction with the first
part of Duodenum.
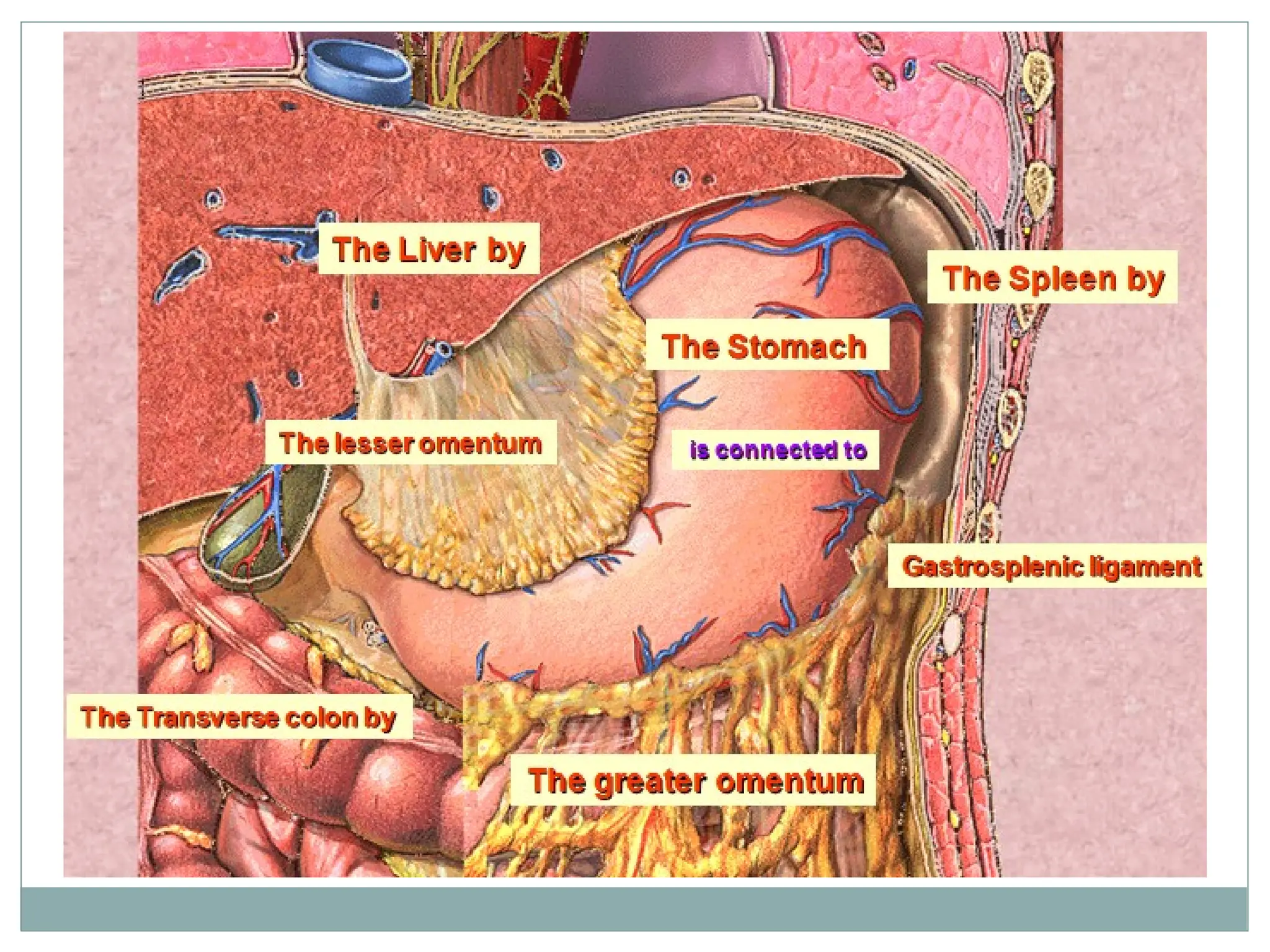
Borders (Curvatures):
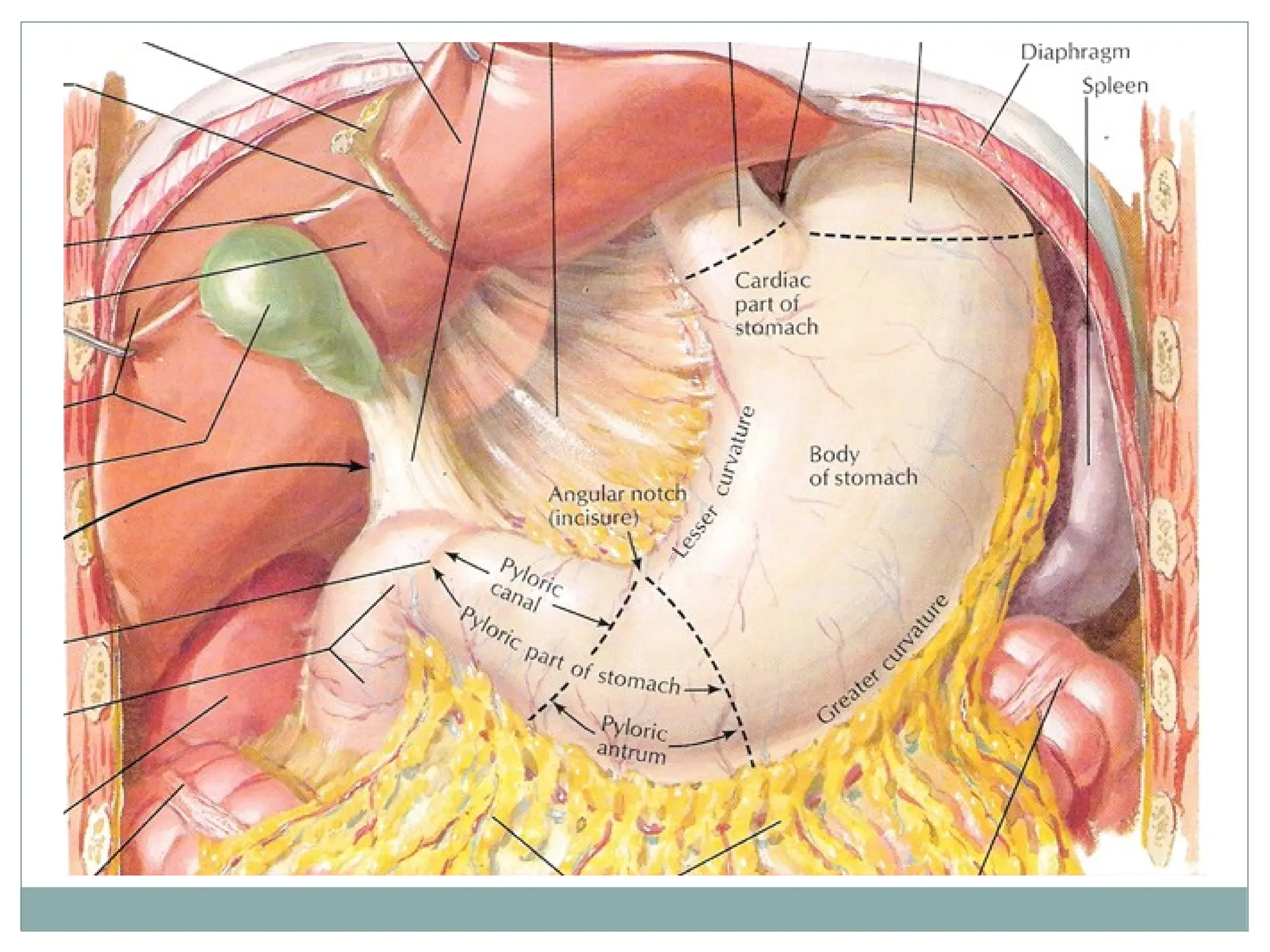
Lesser Curvature (Right Border): Extends from right side of
cardiac end to pyloric end. It is concave. Its maximum concavity is
known as Angular notch (Incisura angularis). It is attached to liver by
lesser omentum.
Greater Curvature (Left Border): Extends from Left side of
cardiac end, follow fundus of stomach to pyloric end. It is convex. It is
attached to spleen by gastrosplenic ligament in upper part and to
transverse colon by greater omentum in the rest of the part.
28.
Features of stomach
Surfaces:
Anterior surface: Between lesser and greater curvature facing
anteriorly.
Posterior surface: Between lesser and greater curvature facing
posteriorly.
29.
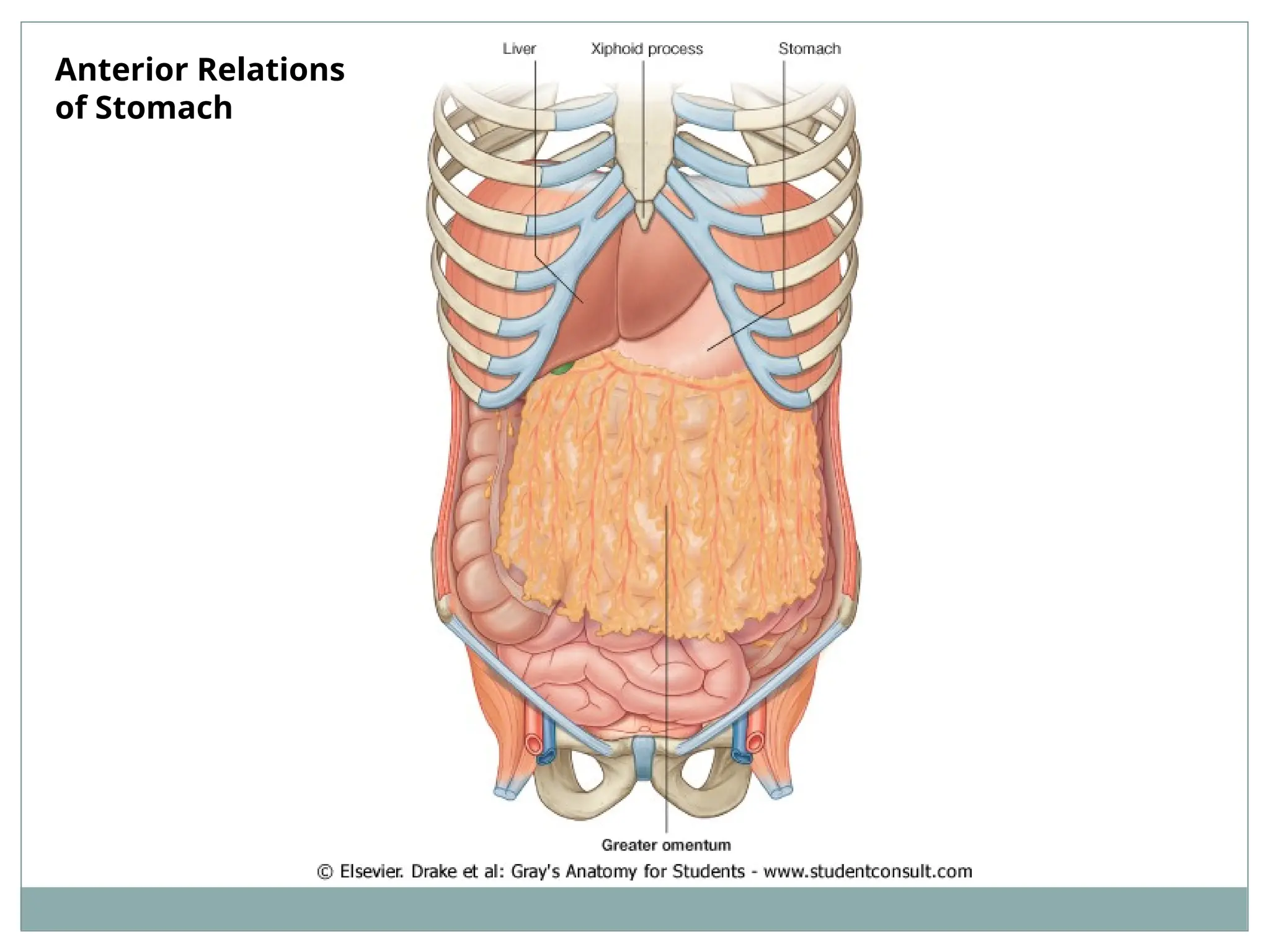
Relations of Stomach
Anterior Surface: covered by peritoneum of
greater sac.
Related to:
Liver ( left lobe and quadrate lobe)
Spleen
Anterior abdominal wall
Diaphragm which separates stomach from left pleura
Relations of Stomach
Structures related to posterior surface also known as Stomach bed and
separated by cavity of lesser sac)
Structures forming stomach bed (Posterior relations):
Left crus of diaphragm
Abdominal aorta
Body of pancreas
Left kidney and left suprarenal gland
Transverse colon and transverse mesocolon
Spleen (separated by cavity of greater sac)
32.
Divisions of stomach
Stomach is divided into two portions by line extending from angular notch of
lesser curvature to the bulge on the greater curvature.
Two portions are:
1. Cardiac portion
2. Pyloric portion
Cardiac portion is subdivided in to two parts by transverse line passing
through cardiac end.
The two parts are:
The fundus: lies above the transverse line and dome shaped.
The body: between transverse line and line from angular notch.
Pyloric portion is subdivided in to two parts by constriction.
The two parts are:
The pyloric antrum: between line from angular notch to constriction.
The pyloric canal (pylorus): Terminal part. 1 inch long. In the wall
contains circular muscle fibers which form pyloric sphincter.
34.
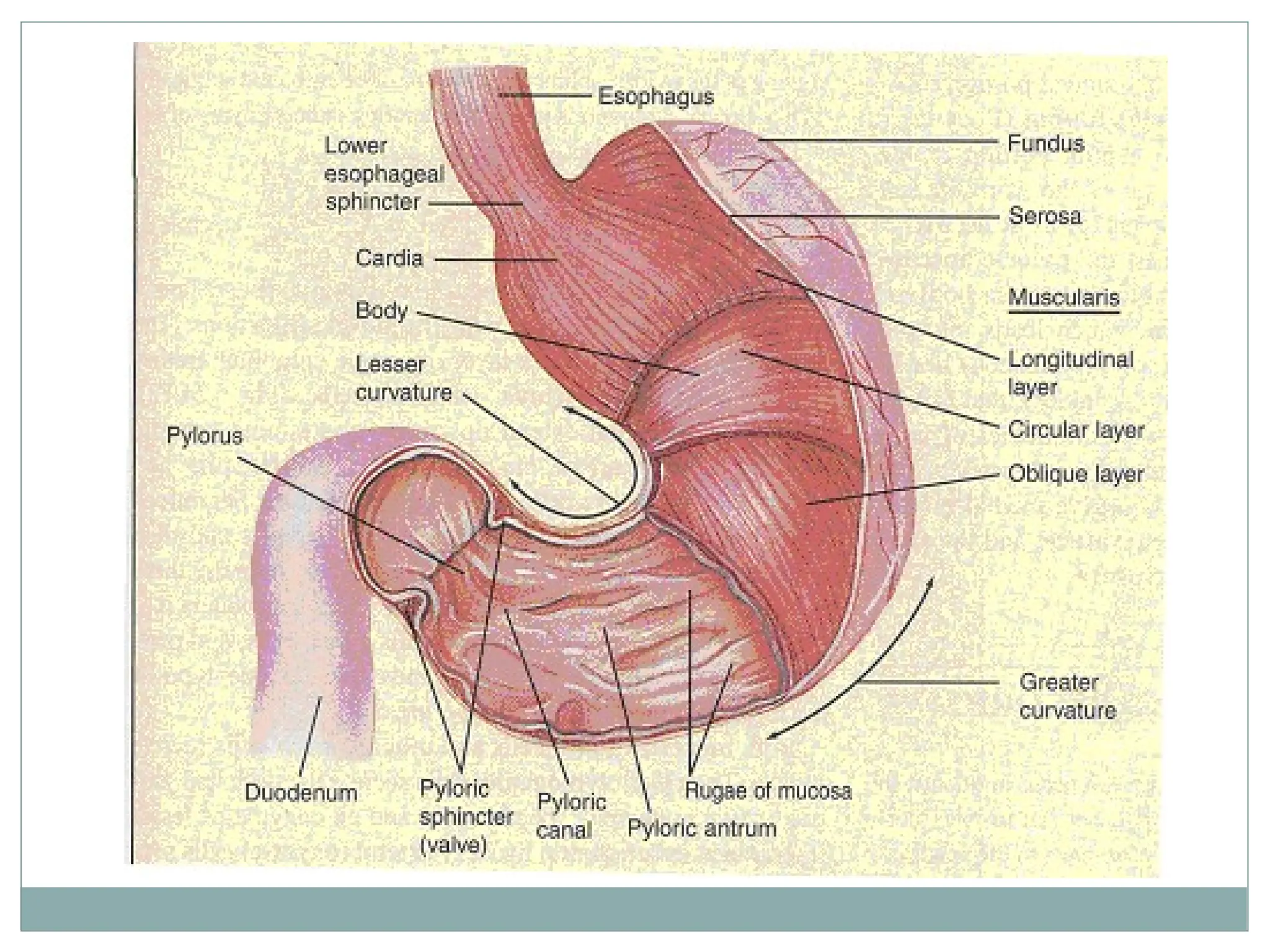
Structure of Stomach
Mucous membrane: thick, vascular and thrown into
folds known as Rugae. Space at the lesser curvature
between prominent longitudinal fold is known as
gastric canal.
Muscular wall: Formed by three layers:
Longitudinal: superficial layer
Circular layer: Middle layer. At pylorus forms pyloric
sphincter.
Oblique: Innermost layer.
36.
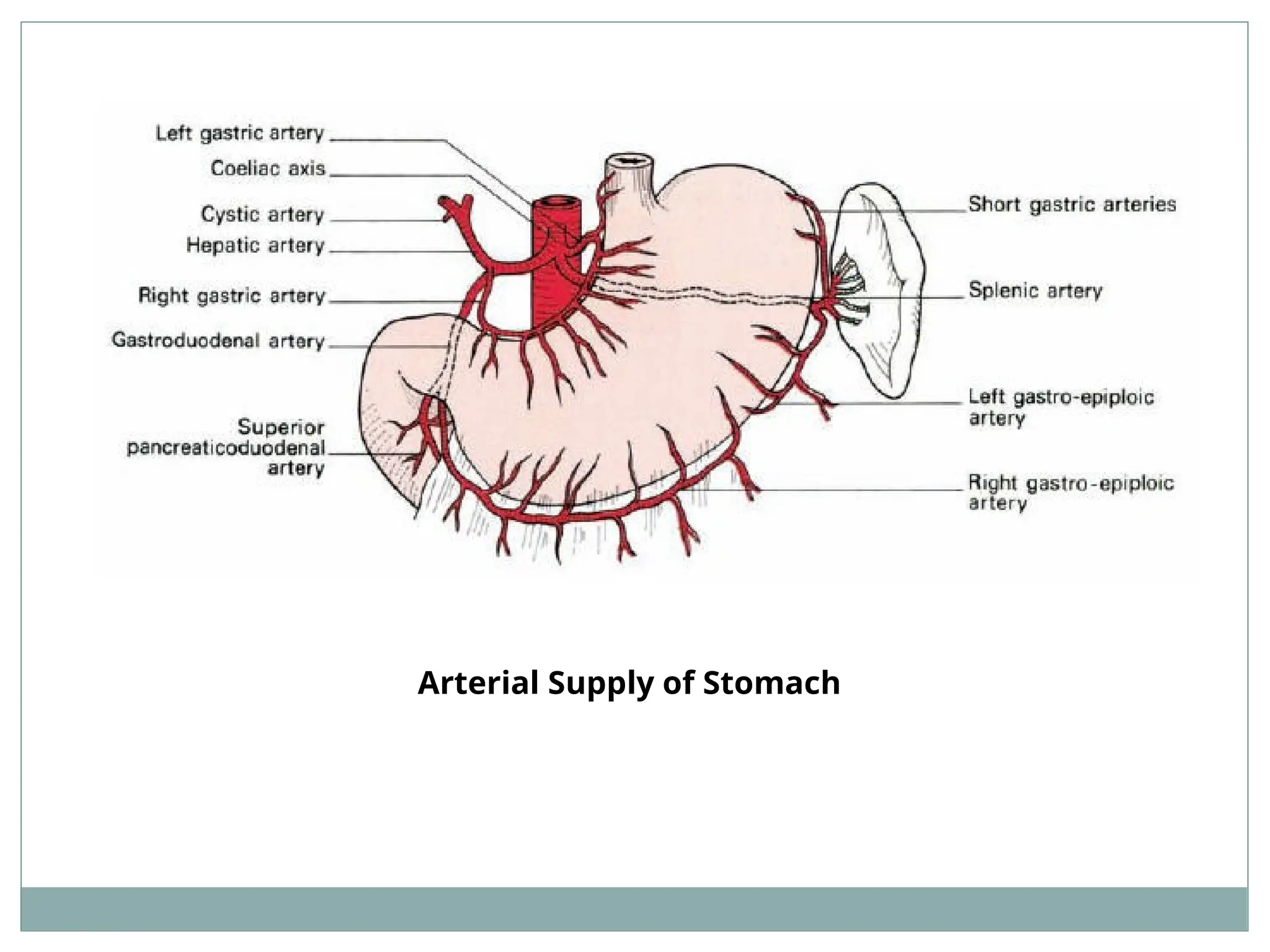
Arterial Supply ofStomach
The stomach is a part of foregut. Hence it is supplied
by branches of Coeliac artery , a branch of
abdomonal aorta.
.
Arterial Supply ofStomach
3. Short gastric arteries: branches of splenic artery (which is
branch of Coeliac artery) at the hilum of spleen . Runs in
gastrosplenic ligament and supplies fundus of stomach.
4. Left gastroepiploic artery: branch of splenic artery (which
is branch of Coeliac artery ) near hilum of spleen. Runs in
gastrospleninc ligament and supplies stomach along greater
curvature.
5. Right gastroepiploic artery: branch from the
gastroduodenal branch of hepatic artery (Which is branch
from coeliac artery). Passes along greater curvature and
supplies lower part of stomach along the greater curvature.
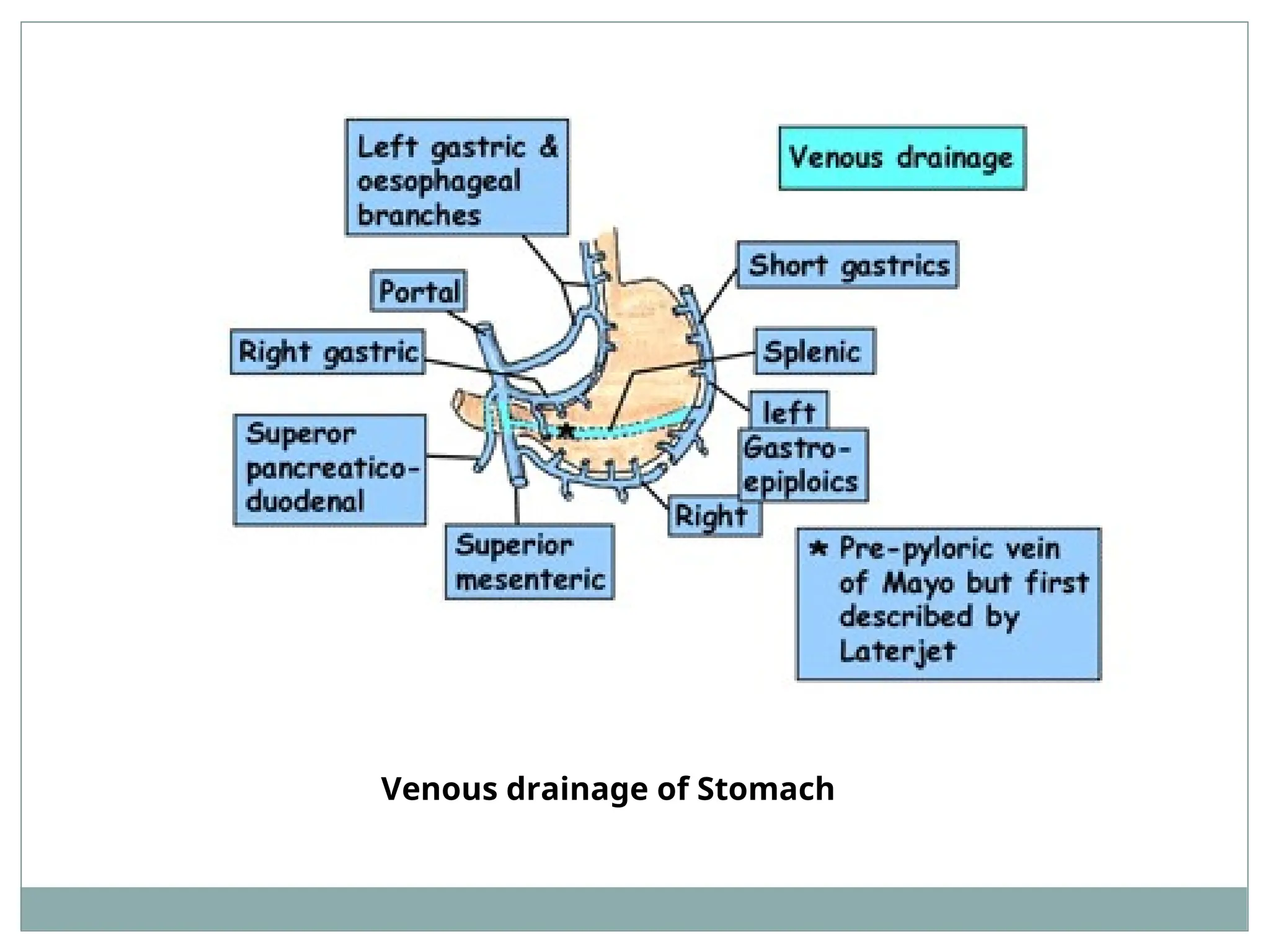
Venous drainage ofstomach
There are 5 veins corresponding to arteries.
All drain into portal system as follows:
Left and right gastric veins into portal vein.
Short gastric and left gastroepiploic vein into splenic
vein.
Right gastroepiploic vein into superior mesenteric
vein.
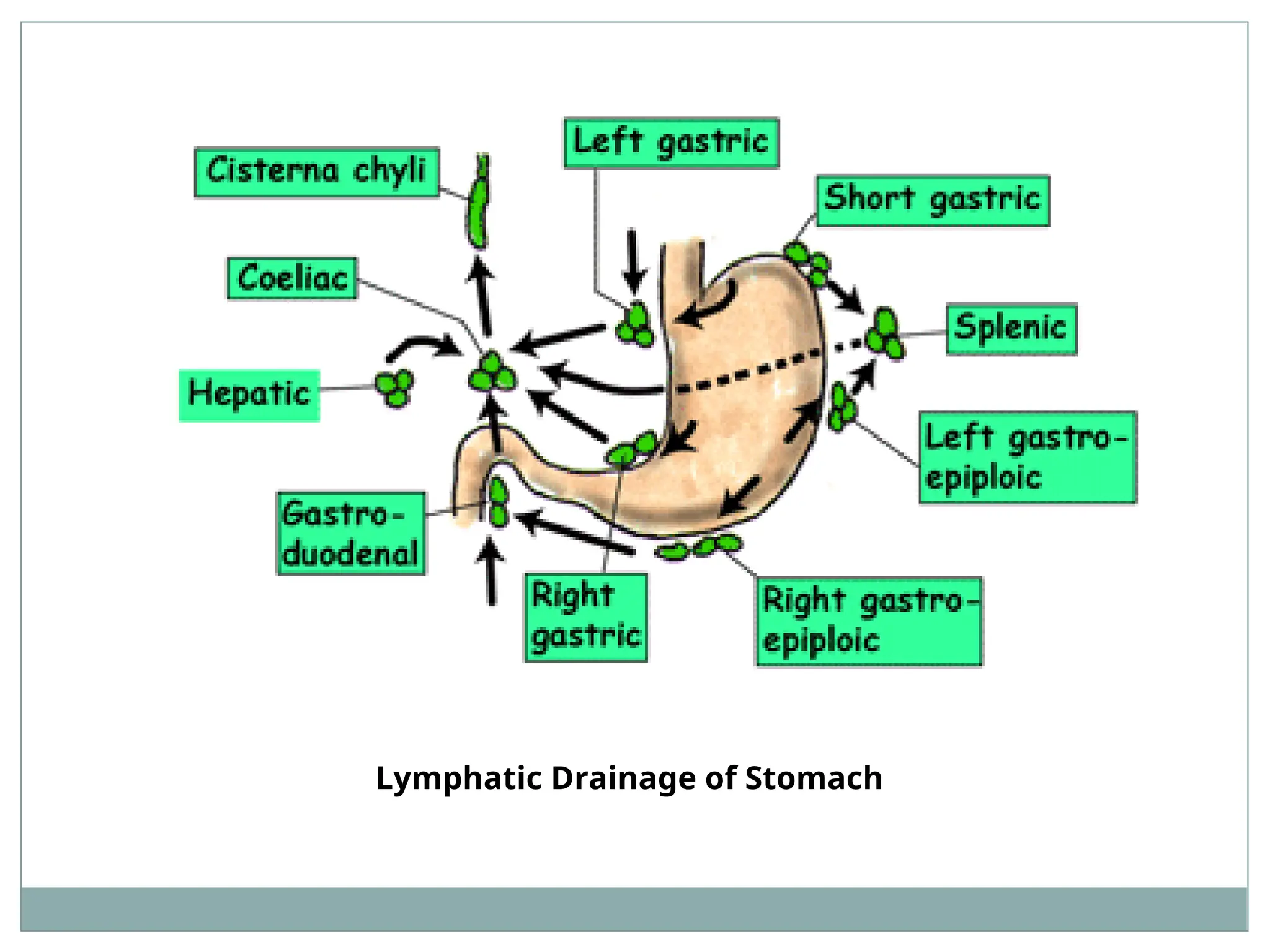
Lymphatic drainage ofstomach
Lymph vessels follow the arteries.
They terminate into right and left gastric and right
and left gastroepiploic lymph nodes.
Efferents from these nodes drain into coeliac lymph
nodes around the root if coeliac artery on posterior
abdominal wall.
Clinical Aspect ofstomach
Gastric ulcer: Most common site at Antrum close to
lesser curvature.
Ulcer on posterior wall may perforate into the lesser
sac and becomes adherent to the pancreas. Erosion
of pancreas cause referred pain on back.
Erosion of splenic artery leads to hemorrahge.
Perforation of ulcer from anterior wall leads to
leakage of contents of stomach in greater sac and
cause peritonitis. It may adhere to liver.
45.
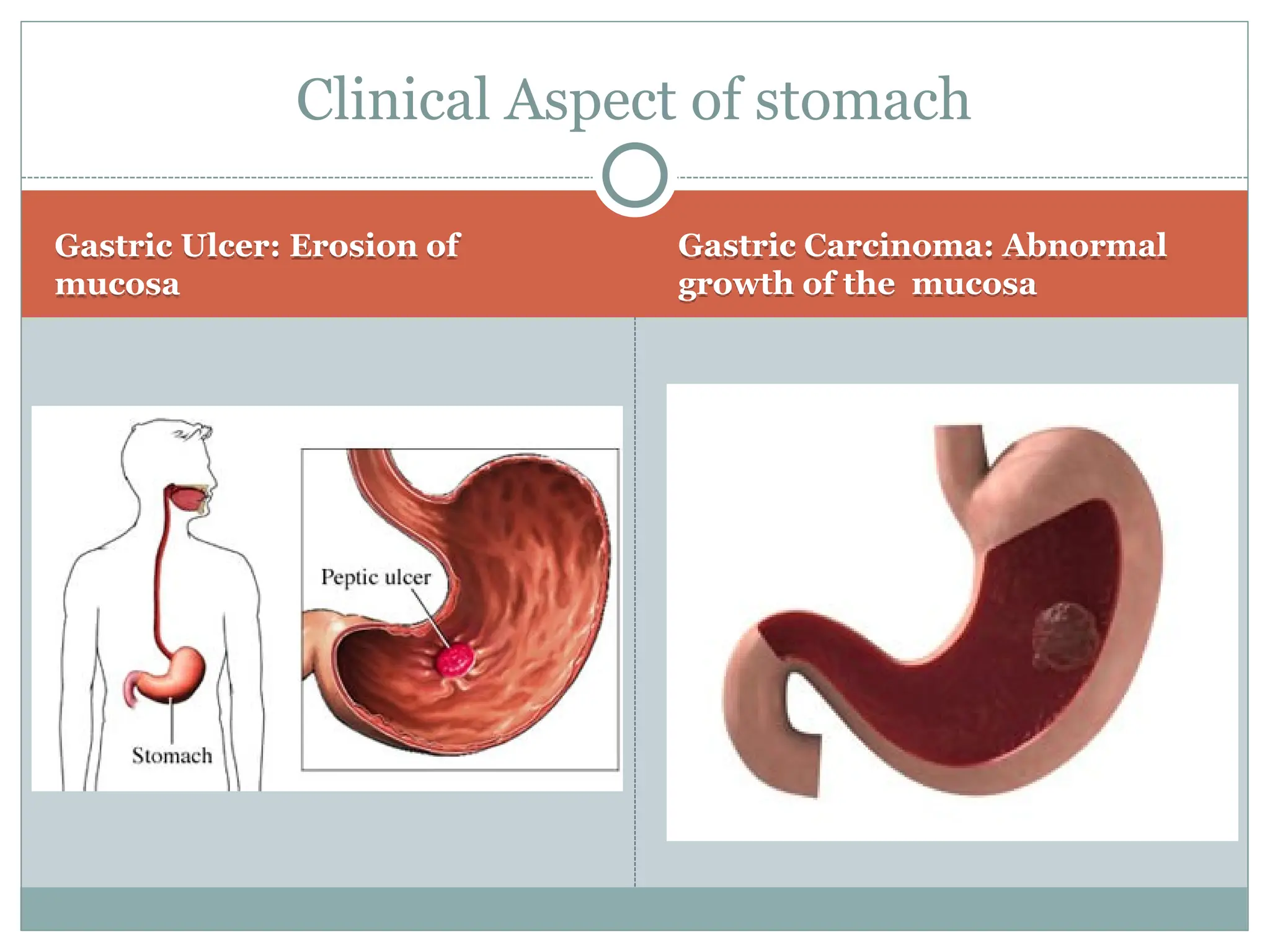
Gastric Ulcer: Erosionof
mucosa
Gastric Carcinoma: Abnormal
growth of the mucosa
Clinical Aspect of stomach
46.
Clinical Aspect ofstomach
Gastric carcinoma: Common at the greater curvature of
stomach.
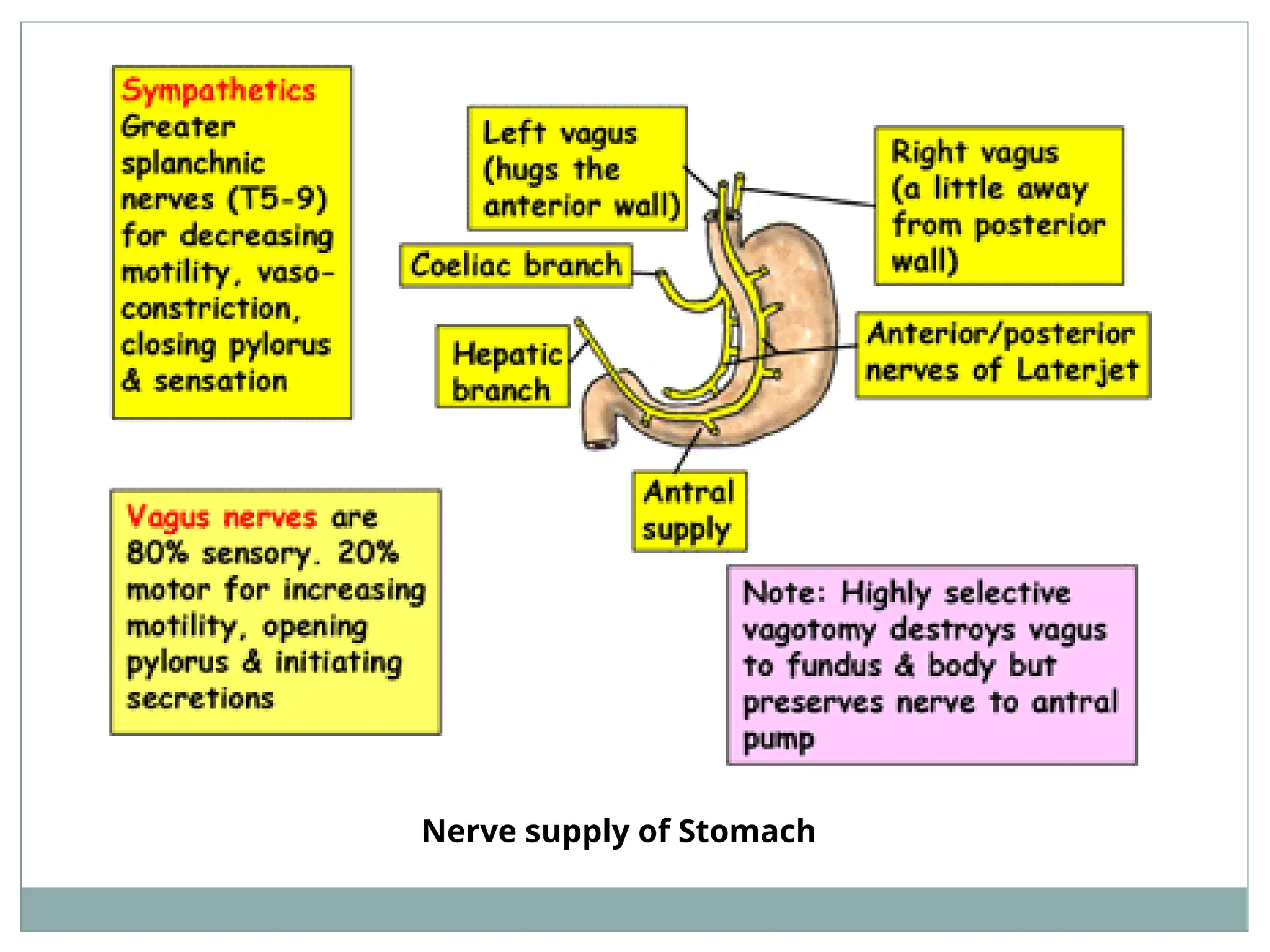
Gastric pain: Caused by stretching of wall (distension) or
spasmodic contraction. Carried by sympathetic nerves
via greater splanchnic nerves to T6-T9 spinal segments.
It is referred to epigastrium.
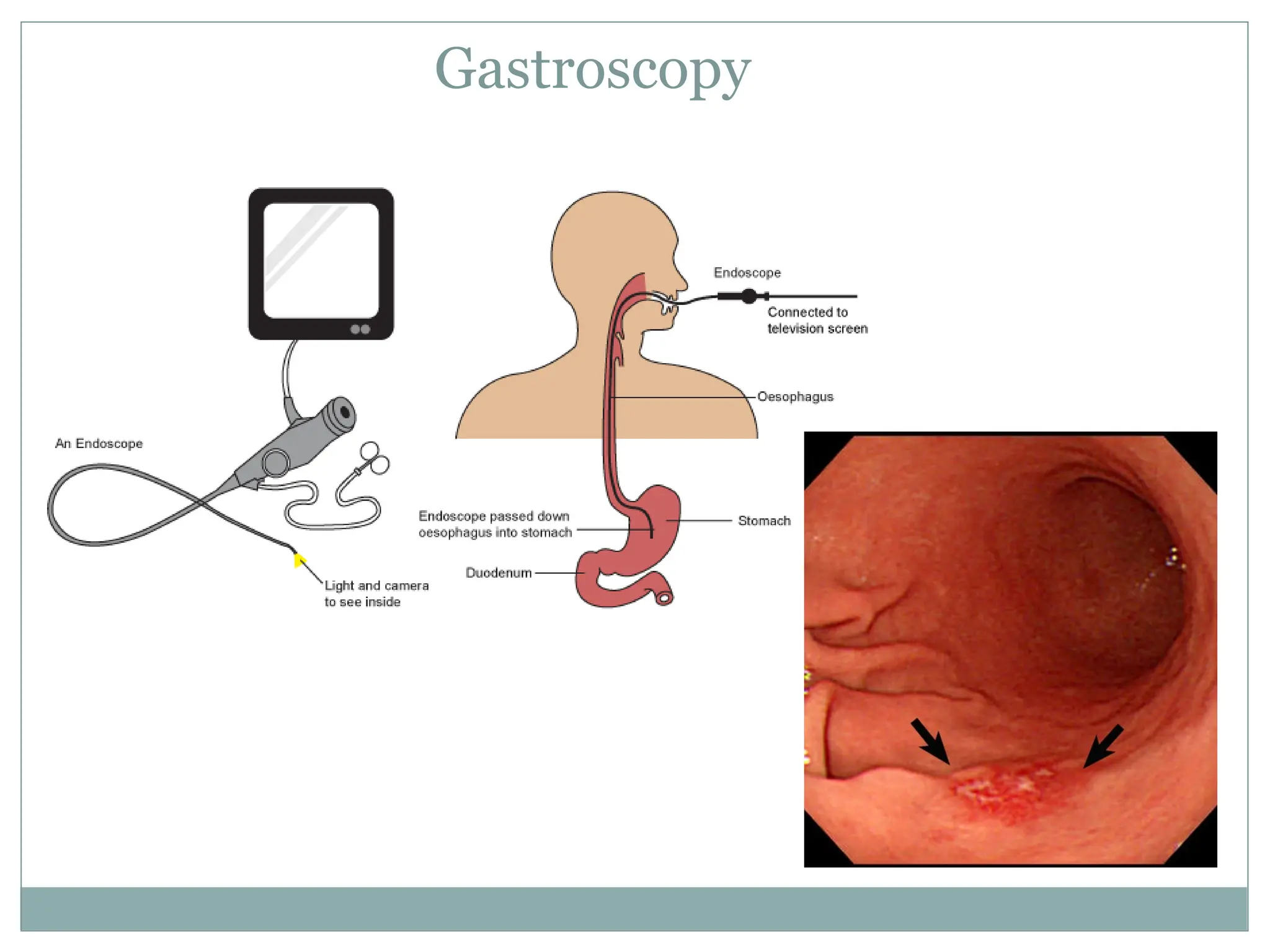
Gastroscopy: direct visualization of stomach by flexible
fibro-optic instrument (Endoscope). It also used to take
mucosal biopsy.
Nasogastric intubation in patients with severe
debilitating illnesses..


























![SURGICAL ANATOMY OF STOMACH [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/surgicalanatomyofstomachautosaved-230608035808-b982958c-thumbnail.jpg?width=640&height=640&fit=bounds)


![Lecture 25 Intermuscular sapces and axilla [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lecture25intermuscularsapcesandaxillaautosaved-251110002658-47b36c78-thumbnail.jpg?width=640&height=640&fit=bounds)






































