Downloaded 911 times
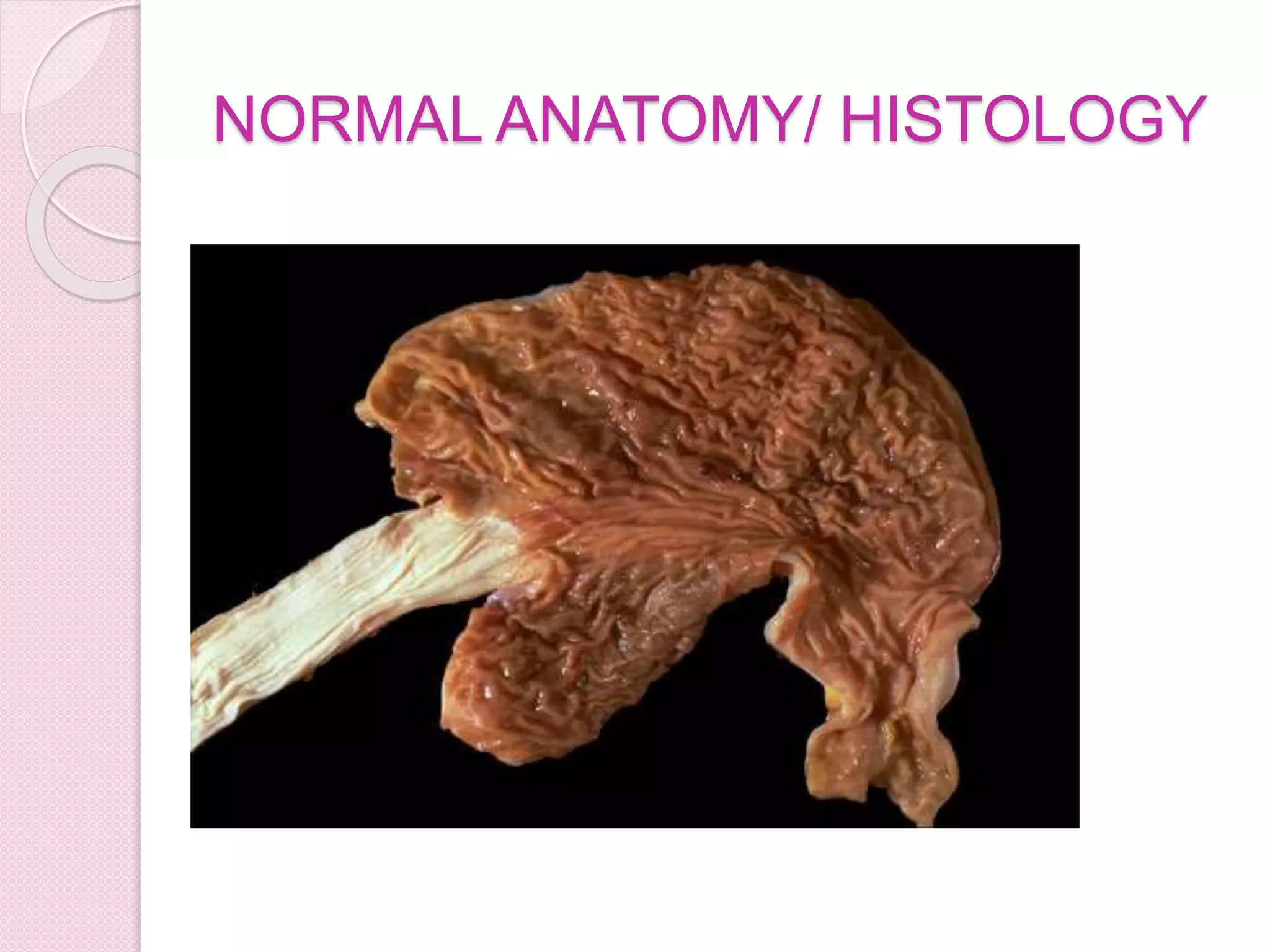
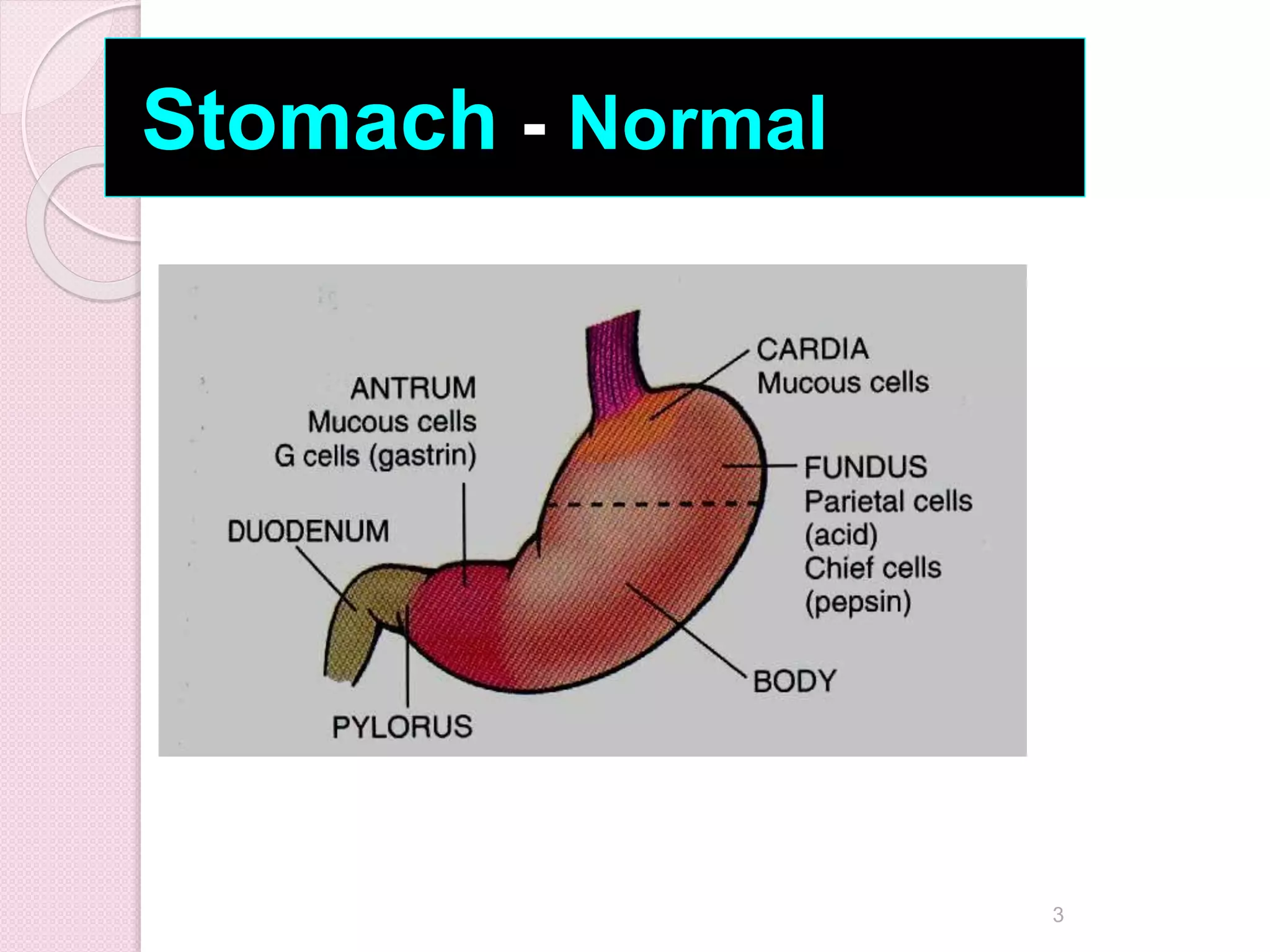
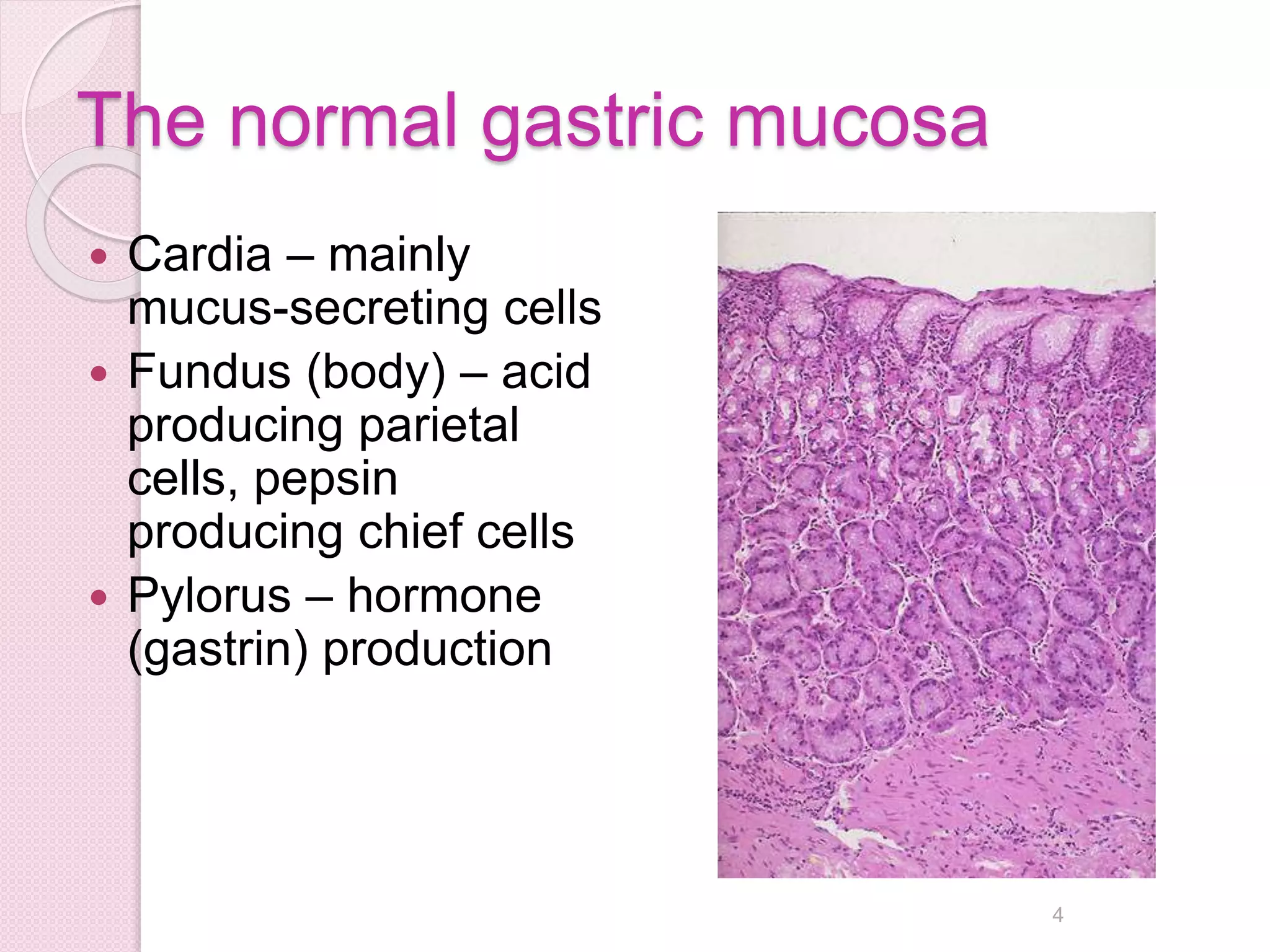
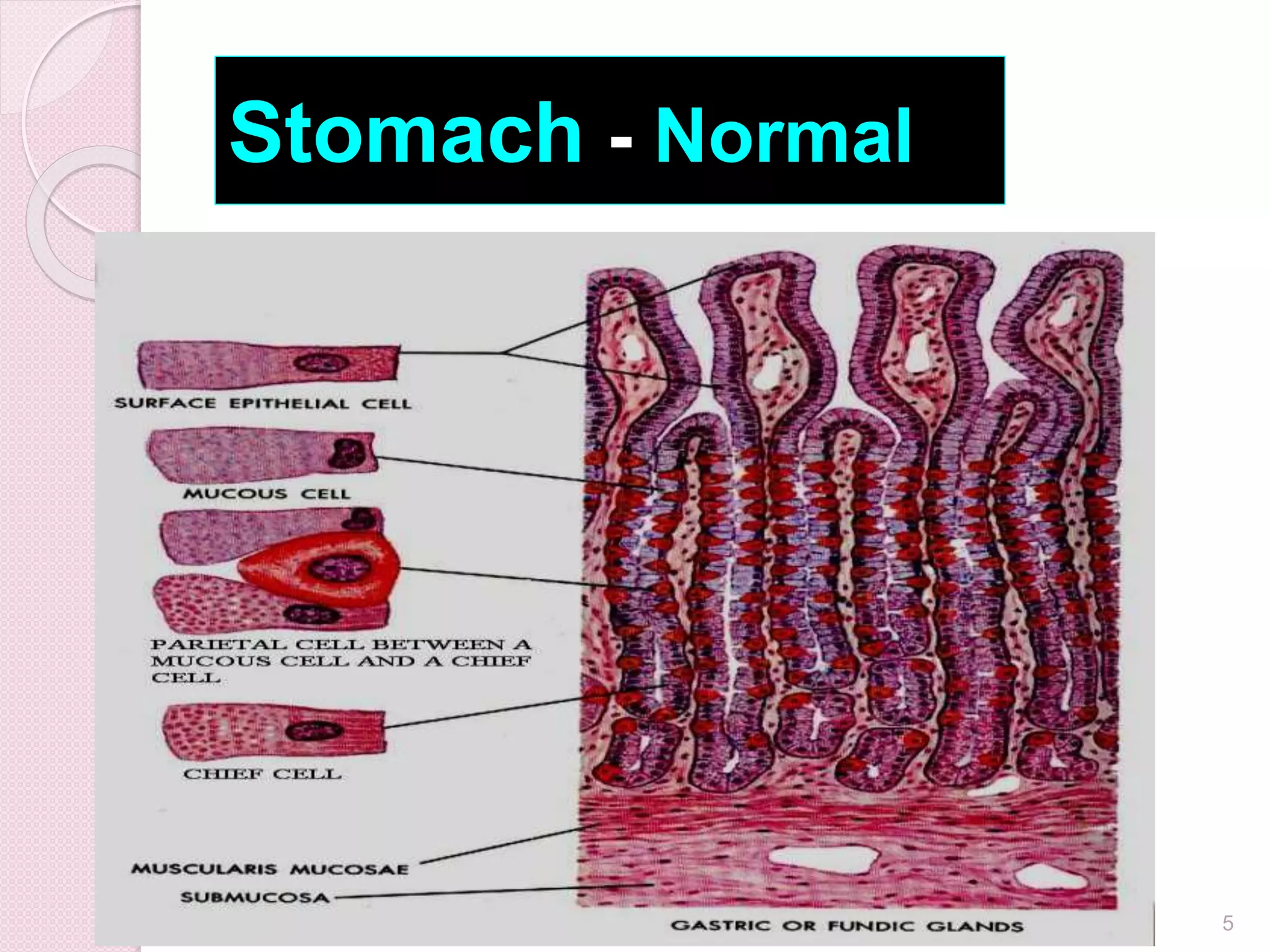
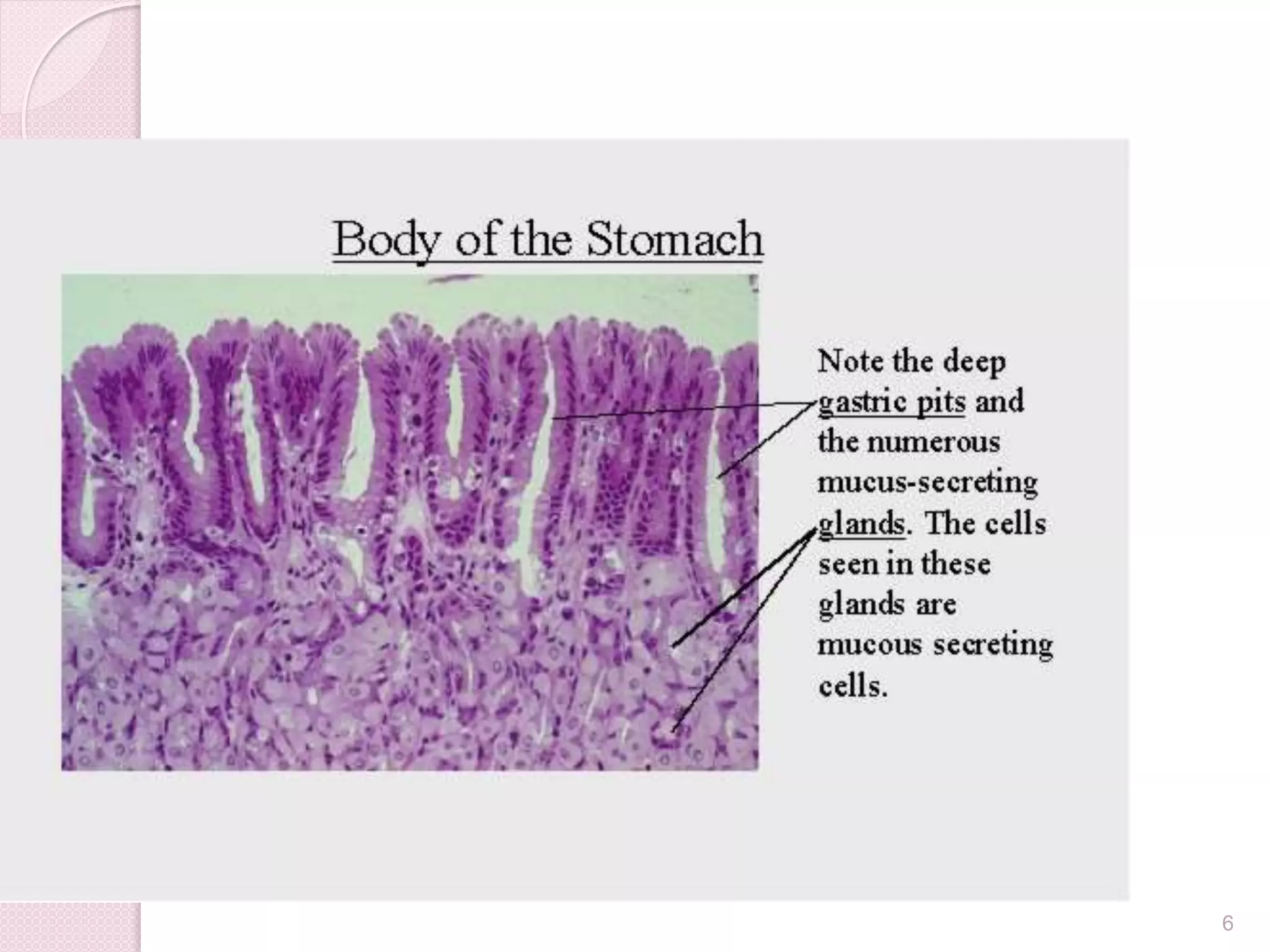
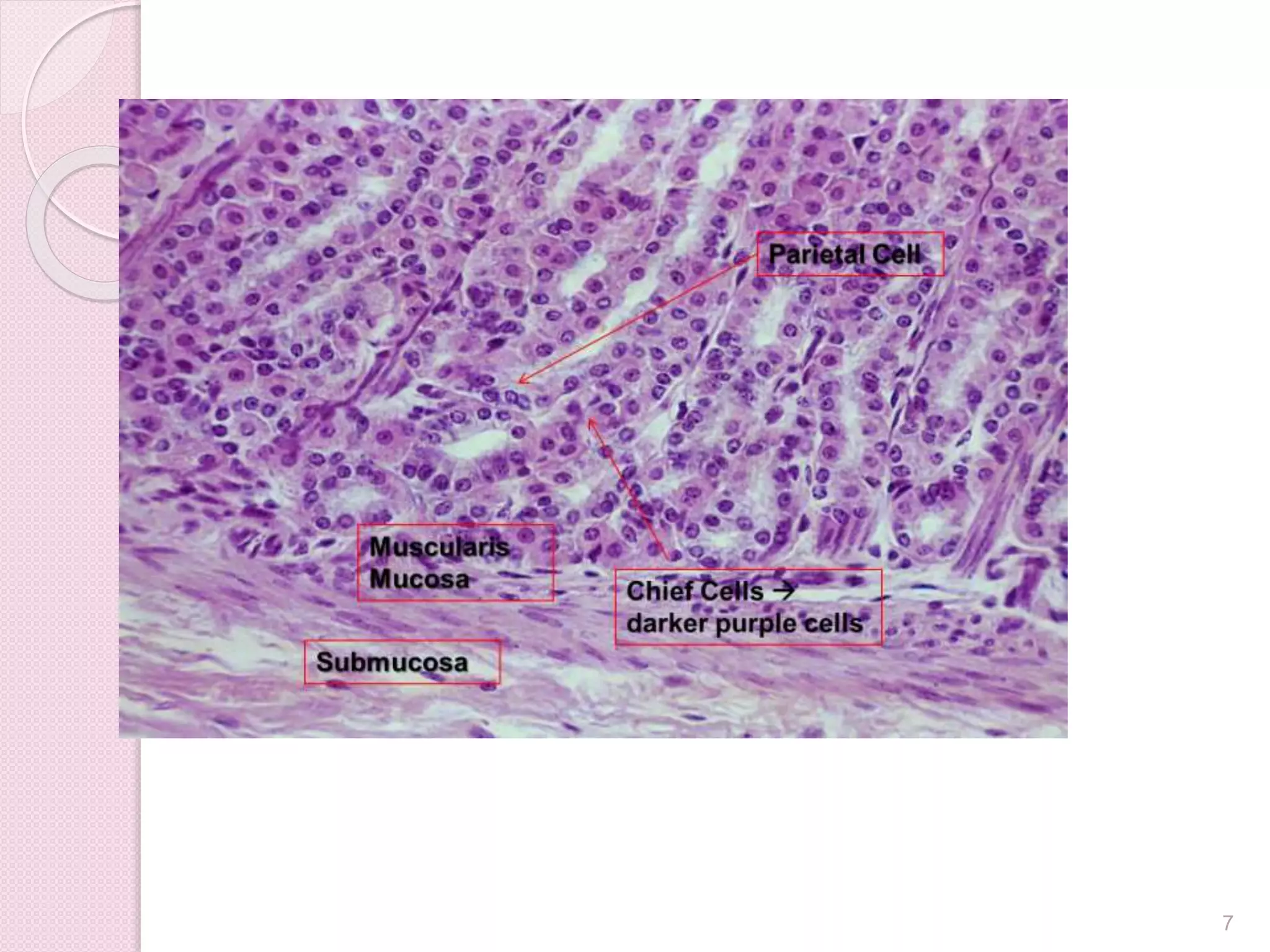
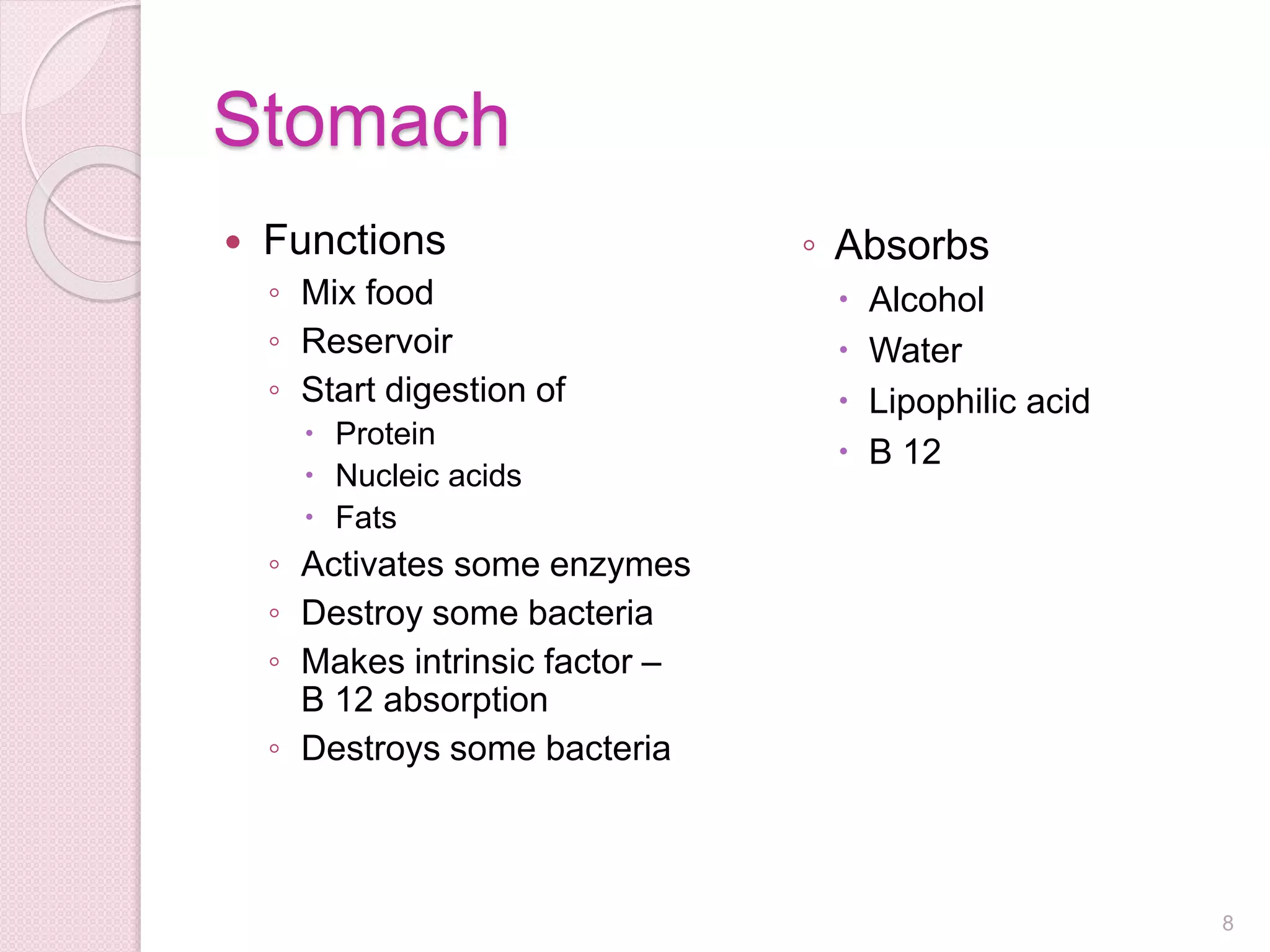











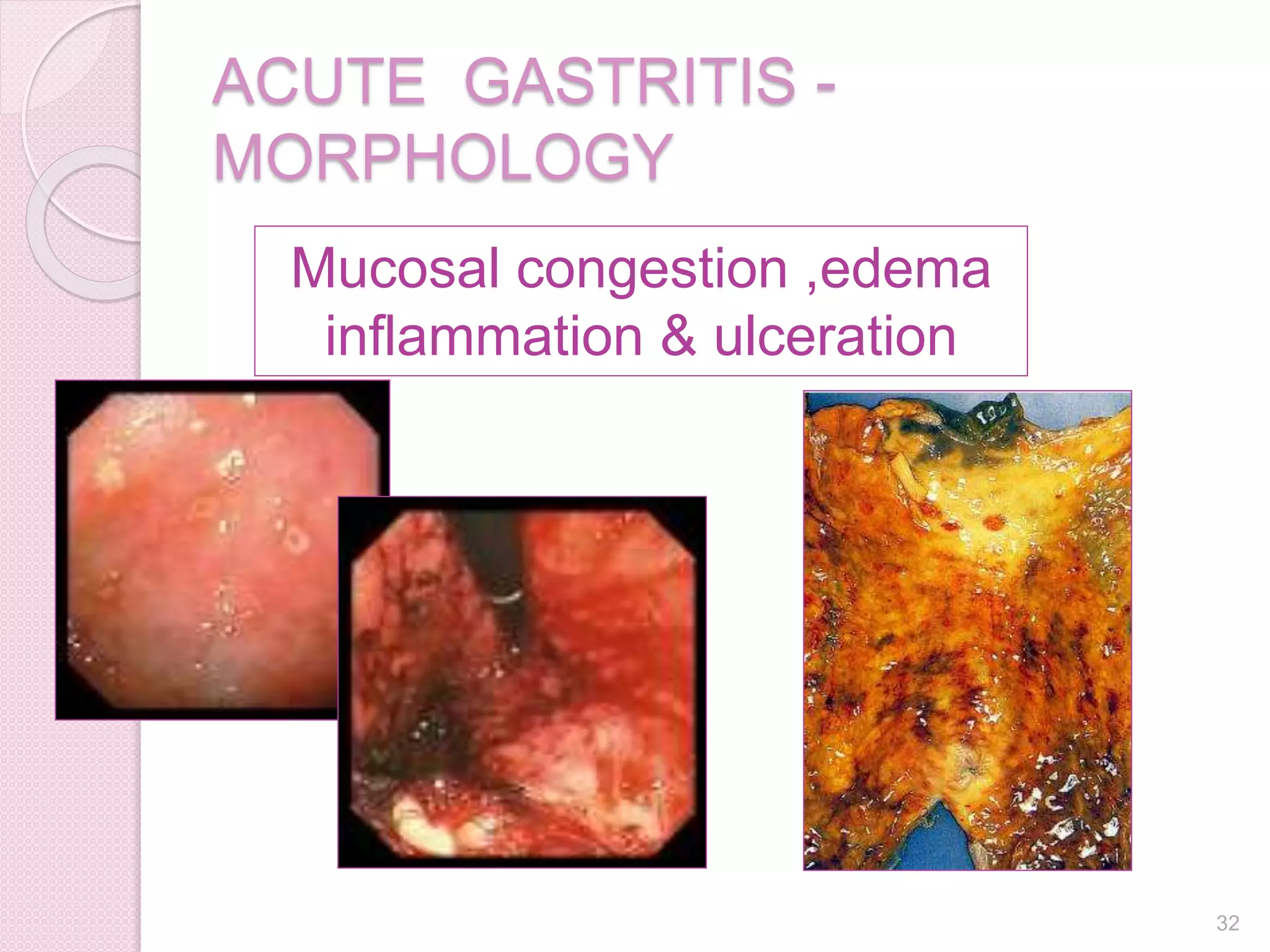

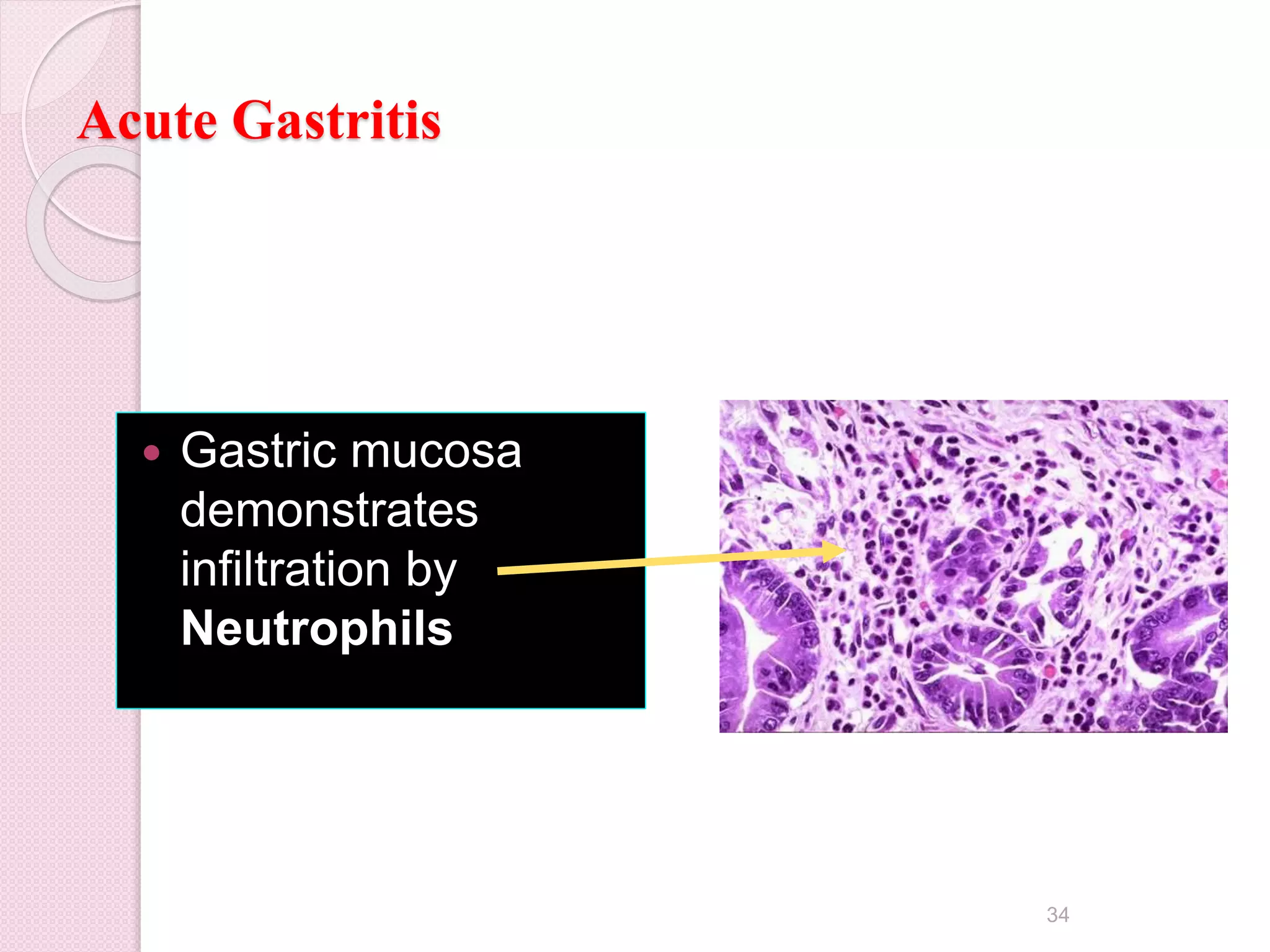




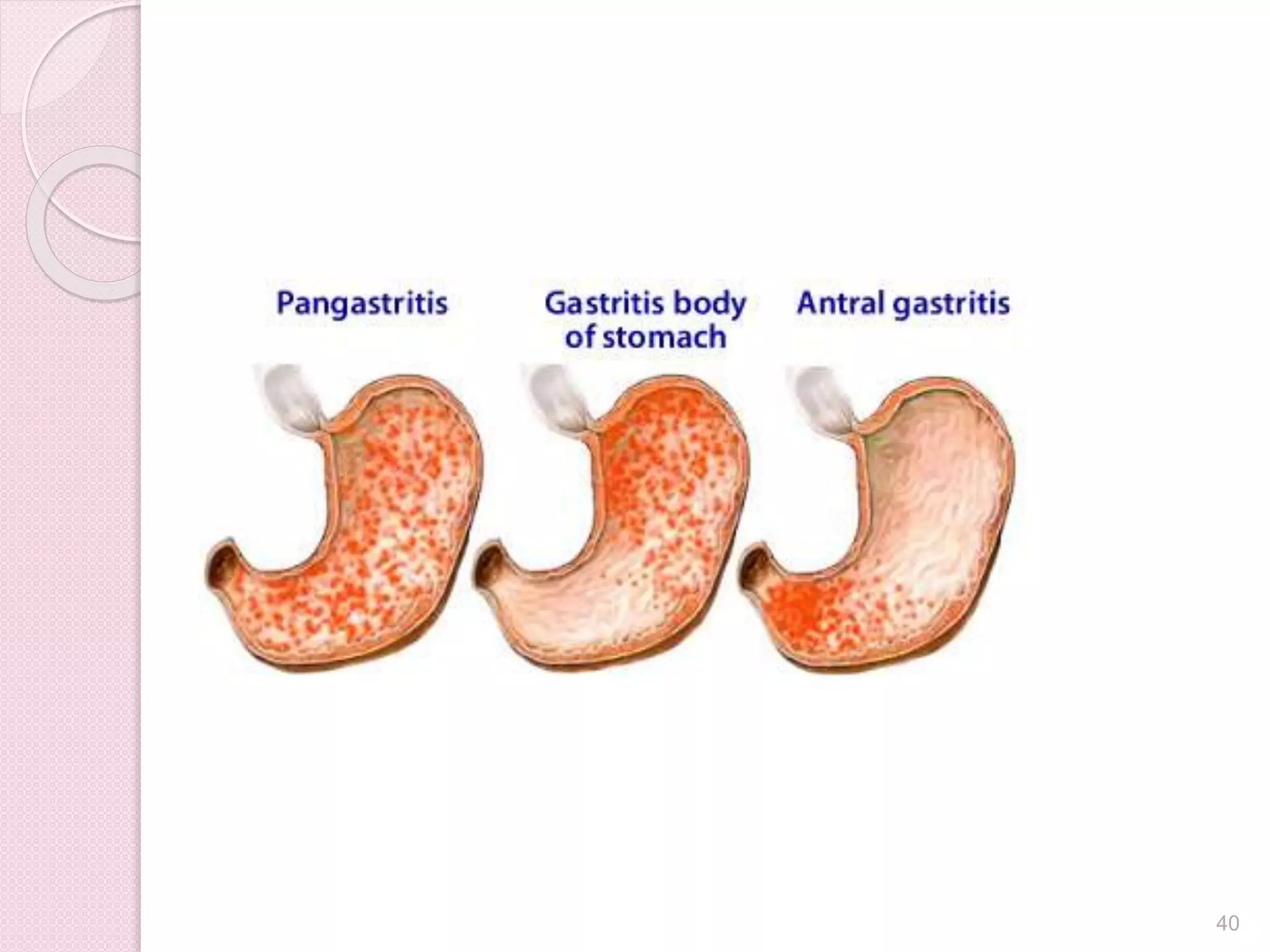


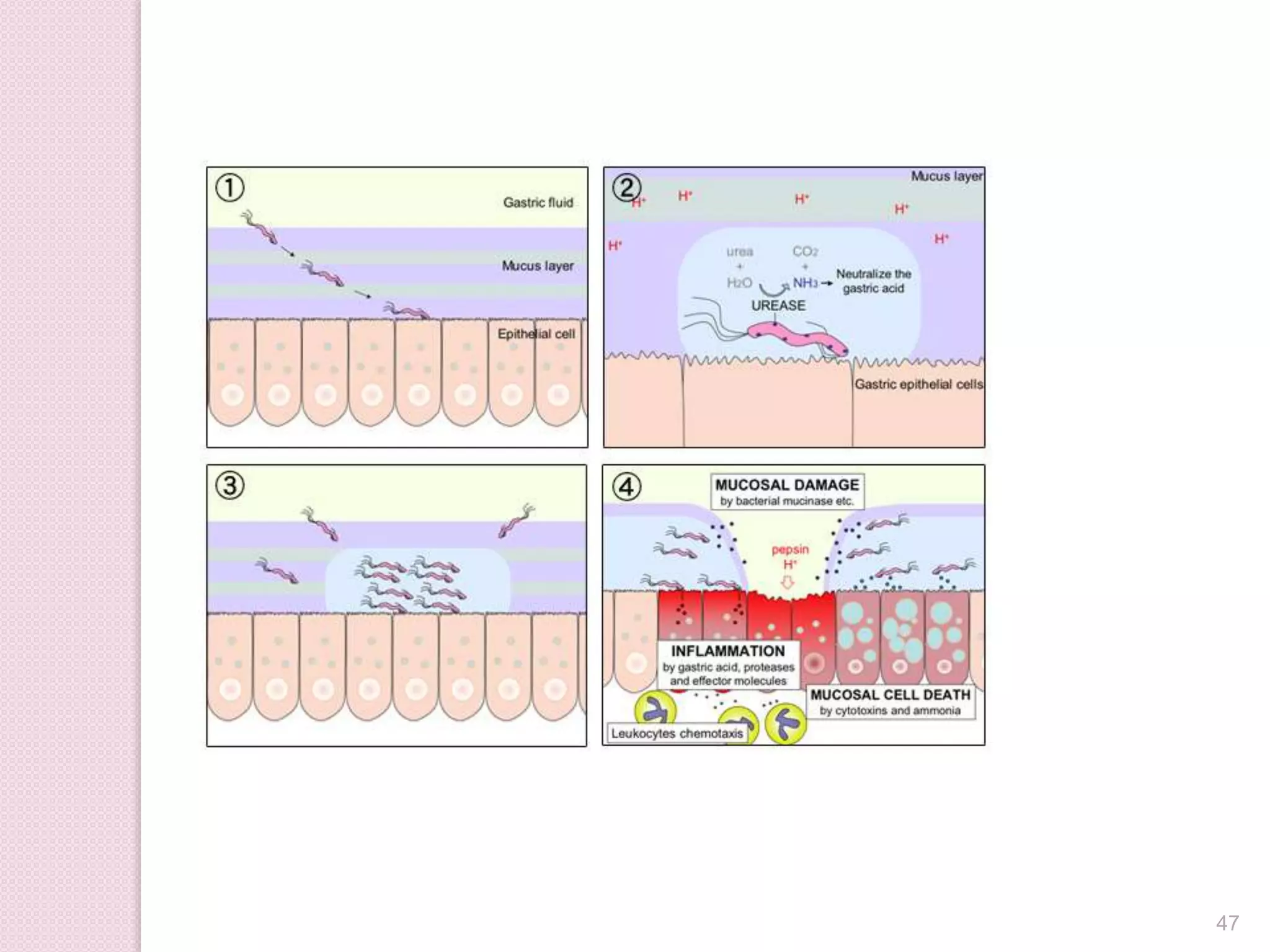


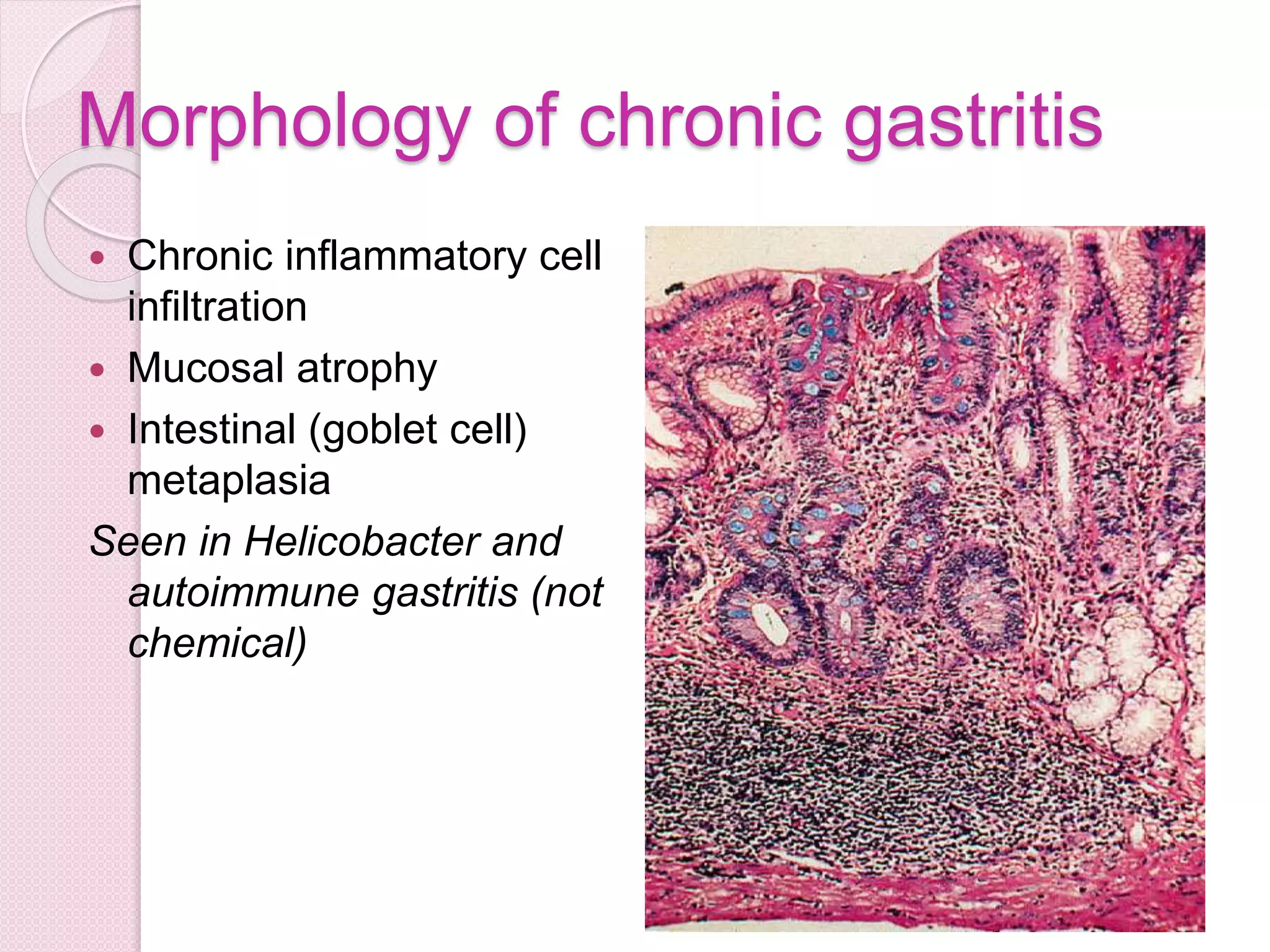







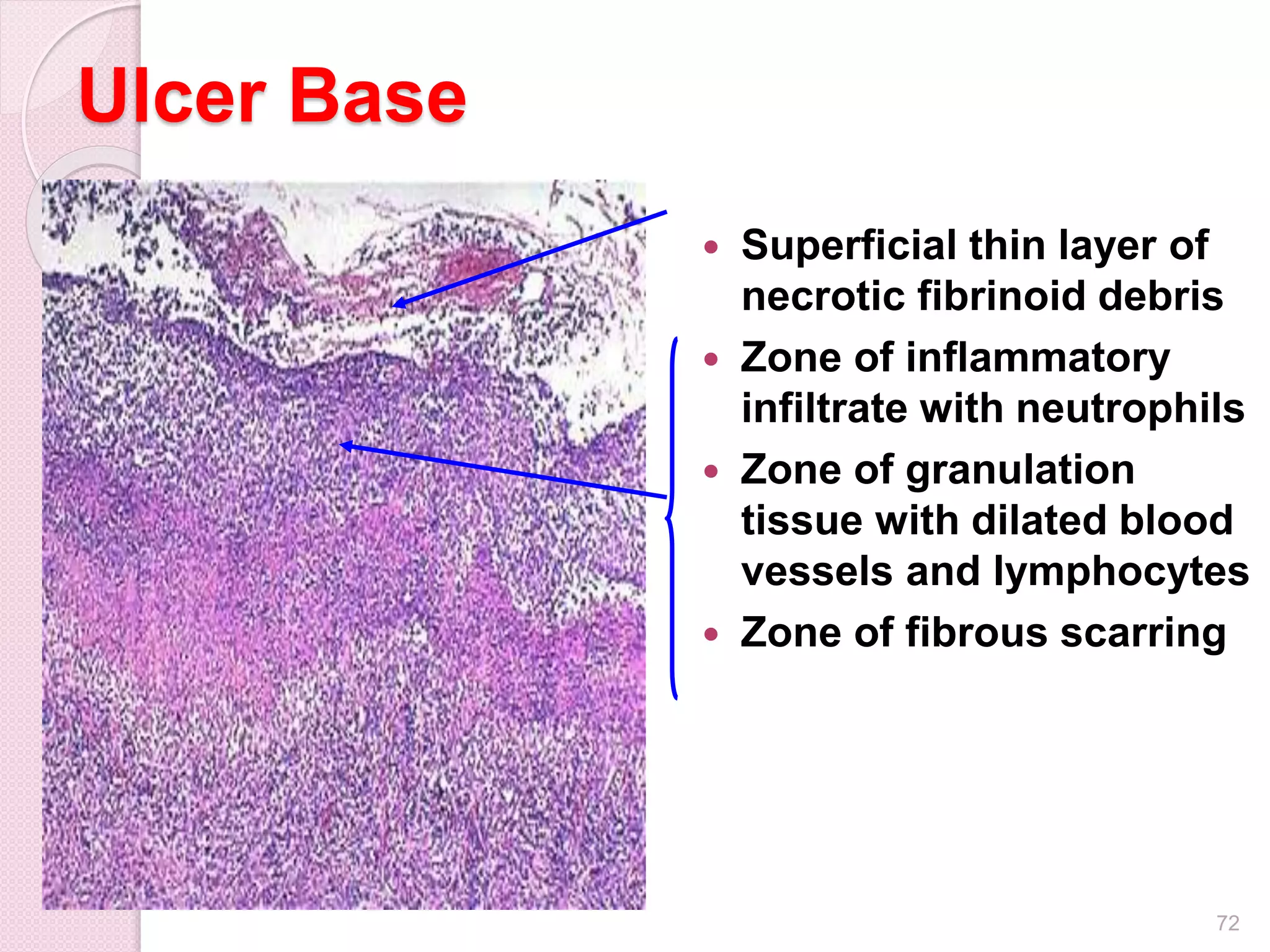

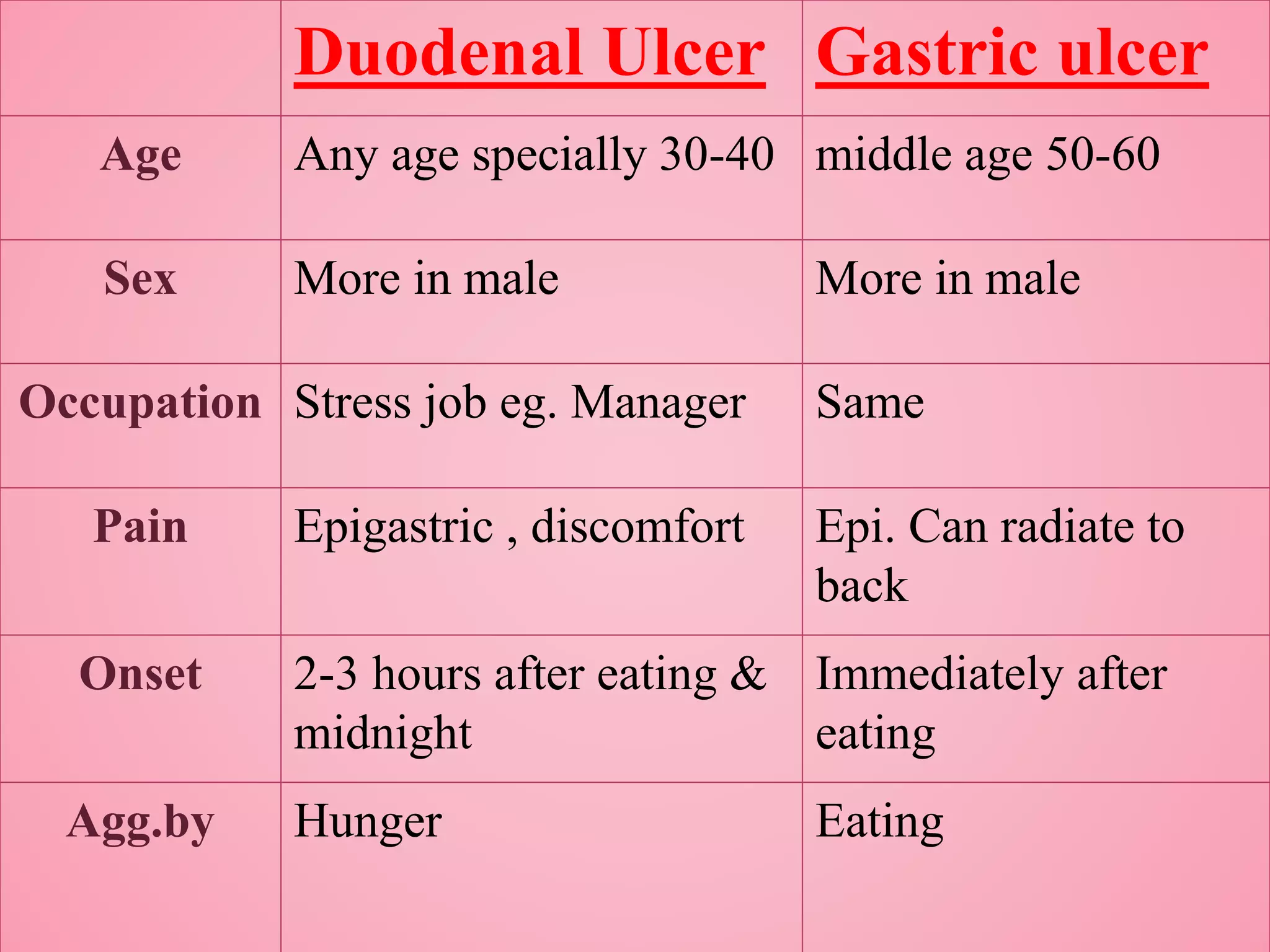

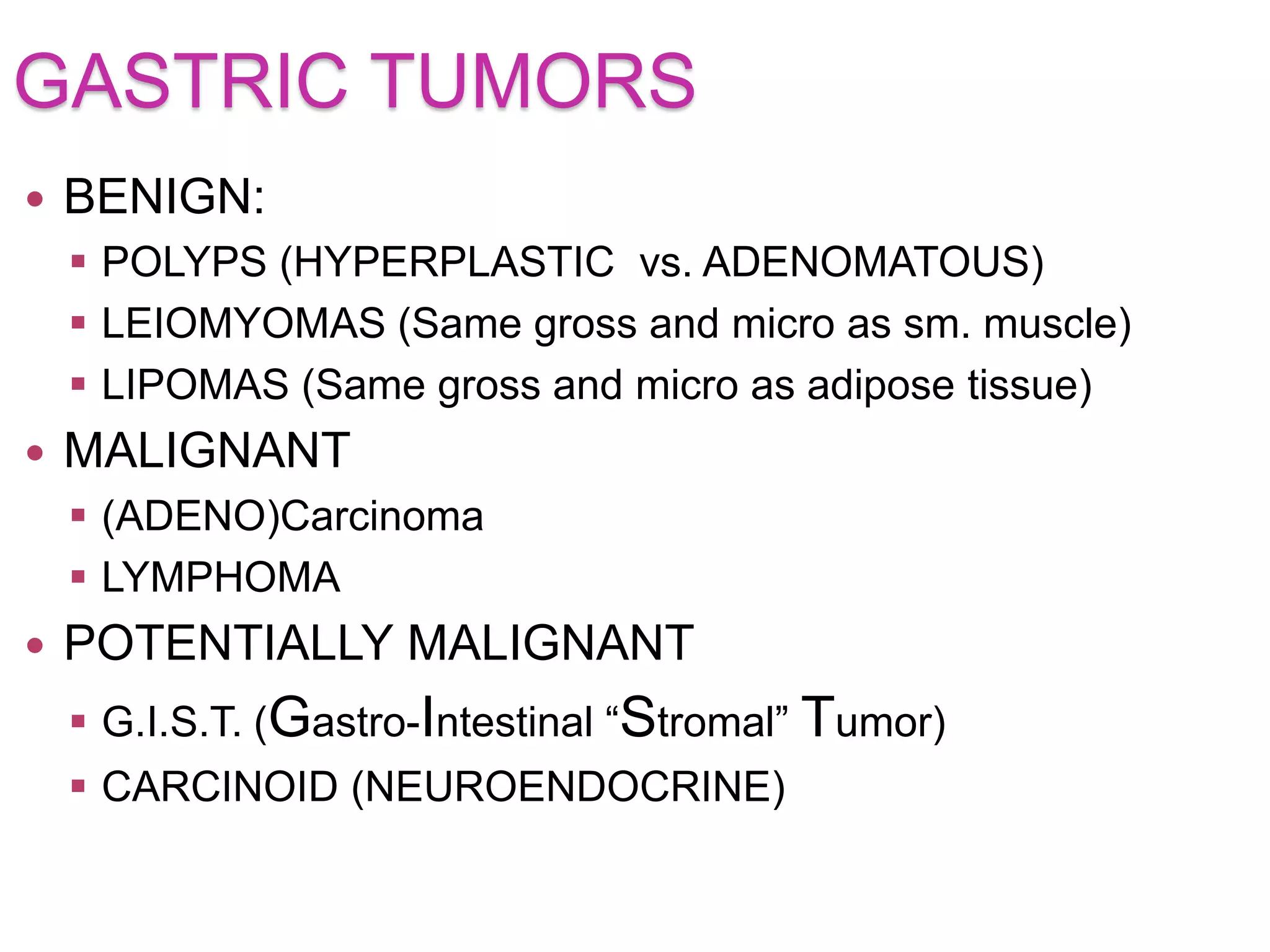
























The normal gastric mucosa contains mucus-secreting cells in the cardia, acid-producing and pepsin-producing cells in the fundus and body, and hormone-producing cells in the pylorus. The stomach functions to mix and start digestion of food, activate enzymes, destroy bacteria, and absorb nutrients, alcohol, water, and vitamins. Common pathologies of the stomach include peptic ulcers, gastritis, tumors, and congenital anomalies like pyloric stenosis. Chronic gastritis is often caused by H. pylori infection and can lead to atrophy, intestinal metaplasia, and increased cancer risk over time if not treated.



























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)







