Download to read offline
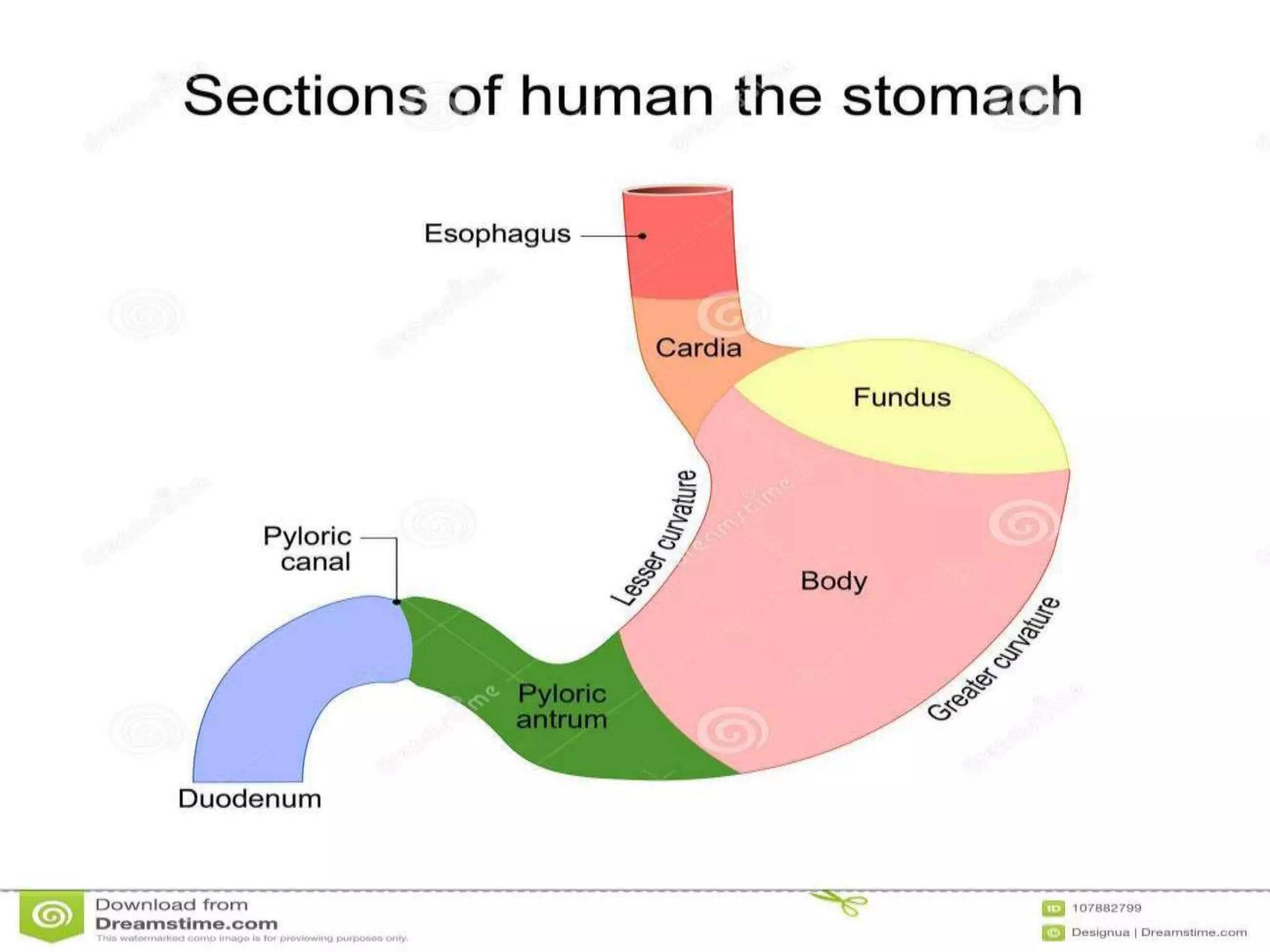




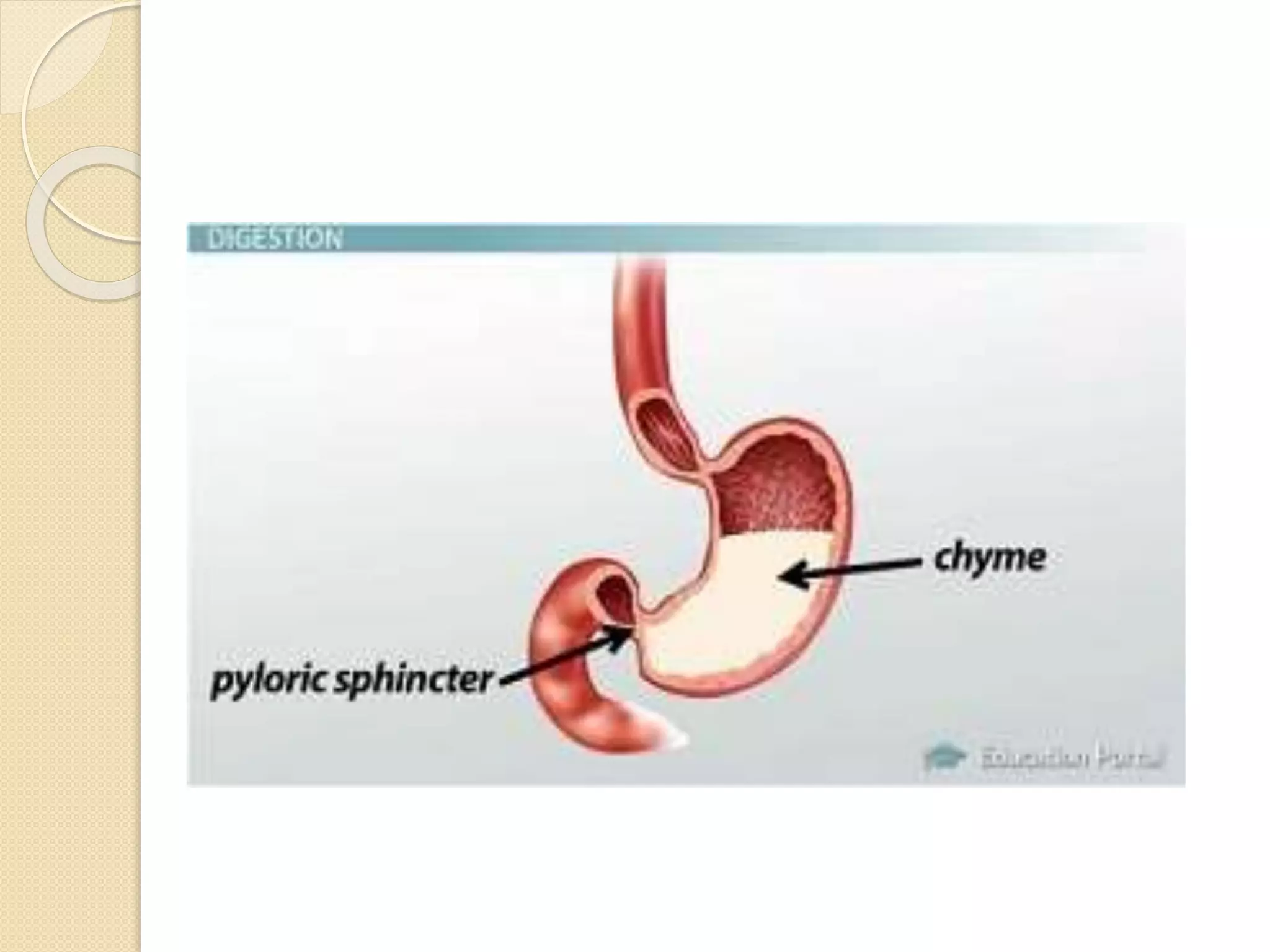

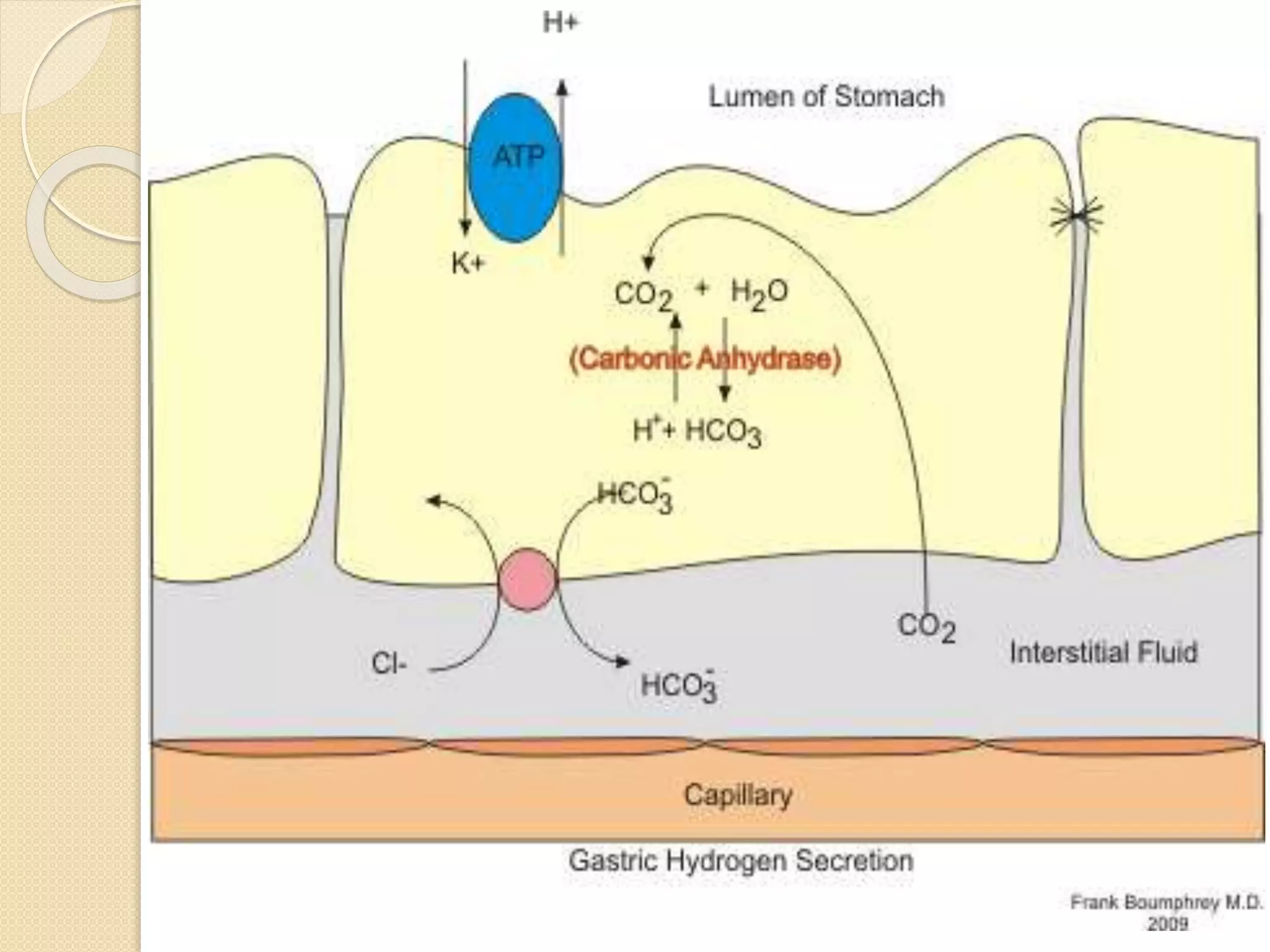

















The stomach has five recognizable parts and two curvatures. Sphincters exist at the entry and exit of the stomach to control movement of contents. The stomach stores food, secretes acid and enzymes to digest food into chyme, and empties at a controlled rate into the small intestine. Acid secretion is stimulated by acetylcholine, gastrin, and histamine in three phases: cephalic, gastric, and intestinal. The stomach mucosa protects itself from acid through secretion of mucus and bicarbonate. Peptic ulcers can form if these defenses are overwhelmed.














































![Stomach by kp [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/stomachbykpautosaved-140422141057-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




















