Download as PDF, PPTX


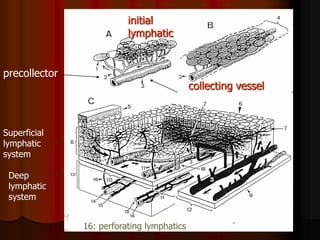
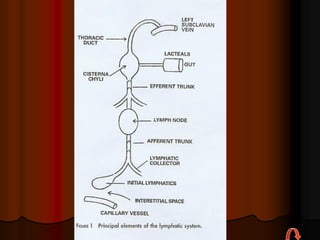
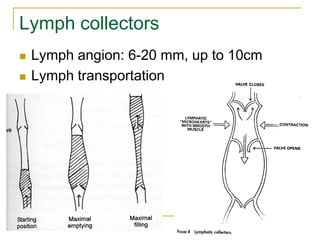
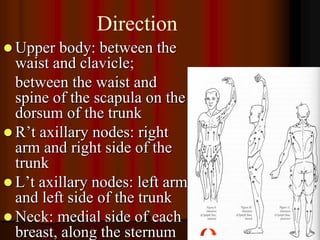
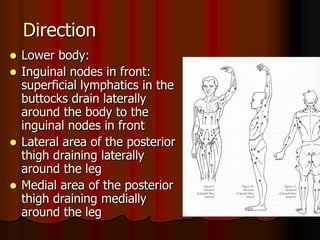




This document provides information on manual lymph drainage for treating lymphedema. It describes the lymphatic system and causes of lymphedema, stages of lymphedema, and complete decongestive physiotherapy. It details techniques for manual lymph drainage including direction of strokes, basic movements like pumps and circles, sequence of treatment, and truncal and extremity drainage patterns. The goal is to encourage lymph flow and reduce swelling through light skin stretching and movement toward lymph nodes.
































































![20131013 03 黃曉峰_安寧緩和照護團隊之決策與溝通 [相容模式]](https://cdn.slidesharecdn.com/ss_thumbnails/2013101303-131030031643-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![20131013 02 翁益強_安寧緩和照護之法律與倫理講義 [相容模式]](https://cdn.slidesharecdn.com/ss_thumbnails/2013101302-131030031642-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)














