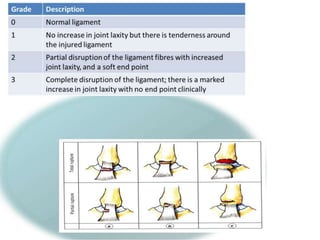
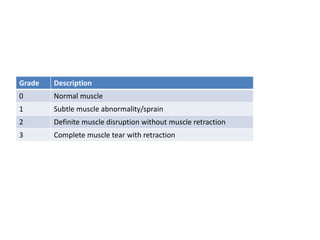
Soft tissue injuries can be acute or chronic and include injuries to muscles, ligaments, and tendons. Acute injuries occur suddenly from trauma while overuse injuries occur gradually. Injuries are classified by degree from mild (grade 1) to severe (grade 3) based on the extent of tissue damage. Treatment focuses on PRICE principles initially followed by rehabilitation exercises to restore strength, mobility, and function. More severe injuries may require surgical intervention.