Total body water(TBW): is approximately
60% of body weight in an adult male.
In a 70 kg man TBW is therefore about 40 L.
the intracellular fluid or ICF
25L
extracellular fluid or ECF
15 L
Among the ECF
interstitial fluid (approximately) 12 L
plasma about
3 L
In the ECF the dominant cation is sodium,
while chloride and, to a lesser extent,
bicarbonate are the most important ECF
12 L 3 L
25 L
3.
The concentration ofsodium in the ECF plays a pivotal role in
determining plasma osmolality and thereby controlling
intracellular volume through changes in water balance
between the intracellular and extracellular space.
In contrast, plasma volume is largely controlled by total body
sodium, which determines volume change.
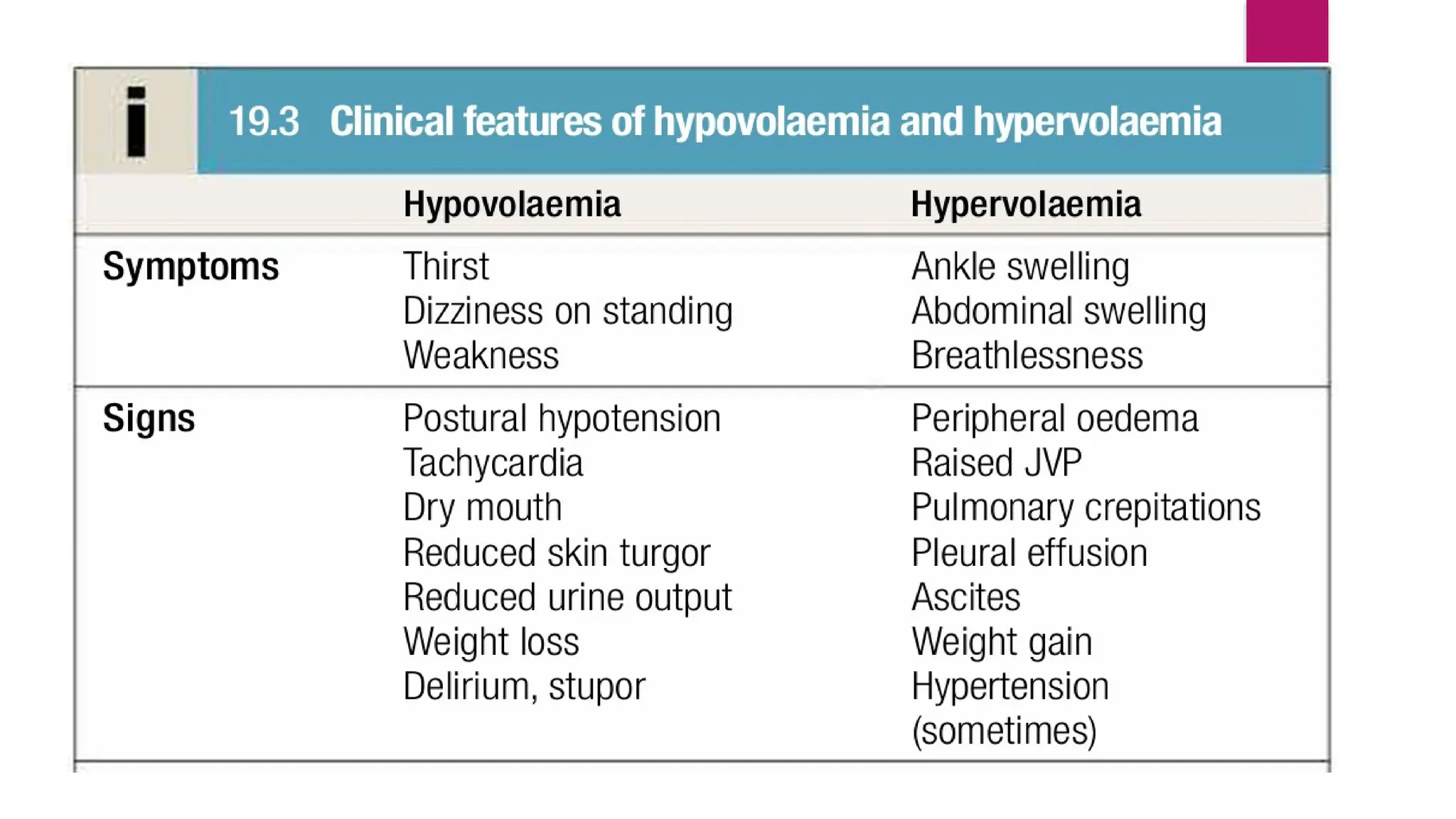
Therefore, disturbances in water homeostasis typically present
with biochemical abnormalities such as hyponatraemia or
hypernatraemia, whereas disturbances in sodium homeostasis
present with hypervolaemia or hypovolaemia.
7.
Daily requirement ofsodium:
1.5-2.0 mmol/kg/day
In a 70 kg adult 105-140 mmol/day
Normal range of serum sodium: 135-145 mmol/L
Hyponatraemia:
Hyponatraemia is definedas a serum Na <135 mmol/L
Pseudohyponatraemia: Artefactual causes of hyponatraemia
should be considered in all cases. These include severe
hyperlipidaemia or hyperproteinaemia, when the aqueous
fraction of the serum specimen is reduced because of the
volume occupied by the macromolecules (although this
artefact is dependent on the assay technology).
Transient hyponatraemia: may also occur due to osmotic shifts
of water out of cells during hyperosmolar states caused by acute
hyperglycaemia or by mannitol infusion, but in these cases
plasma osmolality is normal.
12.
Types of Hyponatraemia:
Onthe basis of duration of onset:
Acute Hyponatraemia - Develops within 48 hrs
Chronic Hyponatraemia - Takes >48hrs to develop
On Biochemical findings/ On the basis of severity:
Mild : 130-135mmol/L.
Moderate : 125-129mmol/L.
Severe : <124mmol/L.
Investigations:
• Serum Electrolytes
•Serum Osmolality
• Urine Electrolytes
• Urine Osmolality
• Serum Protein
• Serum Lipid Profile
• BUN
• Serum Creatinine
• Serum Glucose
• Serum Uric acid
• Serum TSH
• Liver function Test- eg.
Prothrombin
time
• 24hrs Urinary Total Protein
• Chest X ray PA view
• ECG
• Echocardiogram
• CT Scan of Chest & Brain
16.
Management of Hyponatremia:
Hypovolaemic hyponatraemia:
-Oral electrolyte–glucose mixtures
-Increase salt intake
-In a patient with vomiting or severe volume depletion:
Infusion normal saline (0.9% Nacl) with potassium
supplements.
-Treatment of the underlying cause.
17.
Euvolaemic hyponatraemia:
Fluid intake should be restricted to 600-1000ml in 24hrs
In mild sodium deficiency-
-IV infusion of Normal saline (0.9%Nacl) saline.
In case of chronic hyponatremia- correction should be slowly.
Drug induced SIADH- Withdrawal of the offending drug
In prolonged SIADH –oral urea therapy can be given that will
promote water excretion.
Oral vasopressin receptor antagonist- Tolvaptan can be used.
Treatment of the underlying cause eg.- PTB, Brain Tumour etc.
18.
Hypervolaemic hyponatraemia:
Strict fluid restriction with cautious use of diuretics.
Potassium-sparing diuretics may be particularly helpful.
Treatment of the underlying condition eg.- CCF.
In acute onset severe hyponatraemia with signs of
cerebral oedema:
– IV infusion of 3%Nacl
(Initial bolus 150ml over 20 minutes & can be repeated once
or twice depending upon neurological response & rise of
plasma sodium.)
19.
Calculation of totalsodium deficit:
0.6 × weight in kg × (desired Na - actual Na)
A 70 kg adult with 115mmol/L Sodium
Sodium deficit = 0.6x 70 x (135-115) = 0.6 x 70 x 20
= 840 mmol/L
Different preparations of fluids:
3% NaCl ( Hypertonic saline)= 513 mmol/L Na
0.9% NaCl ( Isotonic Saline) = 154 mmol/L Na
The rate of correction of the plasma Na concentration in chronic
asymptomatic hyponatraemia should not exceed 10 mmol/L/24 hrs, and an
even slower rate is generally safer.
Diagnosis:
Low plasmasodium concentration (typically <130mmol/L)
Low plasma osmolality (<275mOsml/kg)
Urine osmolality not minimally low (typically > 100mOsmol/kg)
Urine sodium concentration not minimally low (>30 mmol/L)
Low–normal plasma urea, creatinine, uric acid
Clinical euvolaemia
Absence of adrenal, thyroid, pituitary or renal insufficiency
No recent use of diuretics
Exclusion of other causes of hyponatraemia
Appropriate clinical context:
CXR PA view
CT Scan of chest
CT Scan of brain etc.
22.
Management:
Fluid intakeshould be restricted to 600-1000ml in 24hrs
Drug induced SIADH- Withdrawal of the offending drug
In prolonged SIADH –oral urea therapy can be given that
will promote water excretion
Oral vasopressin receptor antagonist- Tolvaptan can be
used.
23.
Myelinolysis/Osmotic Demyelination Syndrome(ODS):
Rapid correction of sodium in slowly developed
hyponatremia can be hazardous, since brain cells
adapt to slowly developing hypo-osmolality by
reducing the intracellular osmolality, thus maintaining
normal cell volume.
Under these conditions, an abrupt increase in
extracellular osmolality can lead to water shifting out
of neurons.
abruptly reducing their volume and causing them to
detach from their myelin sheaths(‘myelinolysis’)
can produce permanent structural and functional
damage to mid-brain structures (pons) and is
generally fatal.
24.
Clinical Features of
Myelinolysis/OsmoticDemyelination
Syndrome (ODS):
• Confusion
• Dysarthria
• And/or disturbances of conjugate
gaze with out quadriplegia.
In severe form it may present with-
• Pseudobulbar palsy
• Quadriplegia
Investigations:
MRI is useful in establishing the
diagnosis.
25.
So, therapy forthe restoration of severe hyponatremia
should aim for gradual correction,
i.e., by ≤8 mmol/L (8 meq/L) within 24 h
and 15 mmol/L (15 meq/L) within 48 h.
Hypernatraemia: Hypernatraemia isdefined to exist when the serum Na
is >145 mmol/L.
Pathophysiology Hypernatraemia occurs due to inadequate
concentration of the urine in the face of restricted water intake. This can
arise because of failure to generate an adequate medullary
concentration gradient in the kidney due to low GFR or loop diuretic
therapy, but more commonly is caused by failure of the vasopressin
system. This can occur because of pituitary damage (cranial diabetes
insipidus) or because the collecting duct cells are unable to respond to
circulating vasopressin concentrations in the face of restricted water
intake (nephrogenic diabetes insipidus). Whatever the underlying cause,
sustained or severe hypernatraemia generally reflects an impaired thirst
mechanism or responsiveness to thirst.
29.
Clinical features:
• Dizziness
•Delirium
• Weakness
• Ultimately coma and death can result.
Patients with hypernatraemia generaly have
reduced cerebral function, which results in dehydration of
neurons and brain shrinkage.
Management:
Treatment of hypernatraemiadepends on both the rate of
development and the underlying cause.
If the condition has developed rapidly, neuronal shrinkage may be
acute and relatively rapid correction may be attempted. This can
be achieved by infusing an appropriate volume of intravenous
fluid (isotonic 5% dextrose or hypotonic 0.45% saline).
In older, institutionalised patients, it is more likely that the disorder
has developed slowly, and extreme caution should be exercised in
lowering plasma sodium to avoid the risk of cerebral oedema.
The underlying cause should also be addressed.