Download as PDF, PPTX


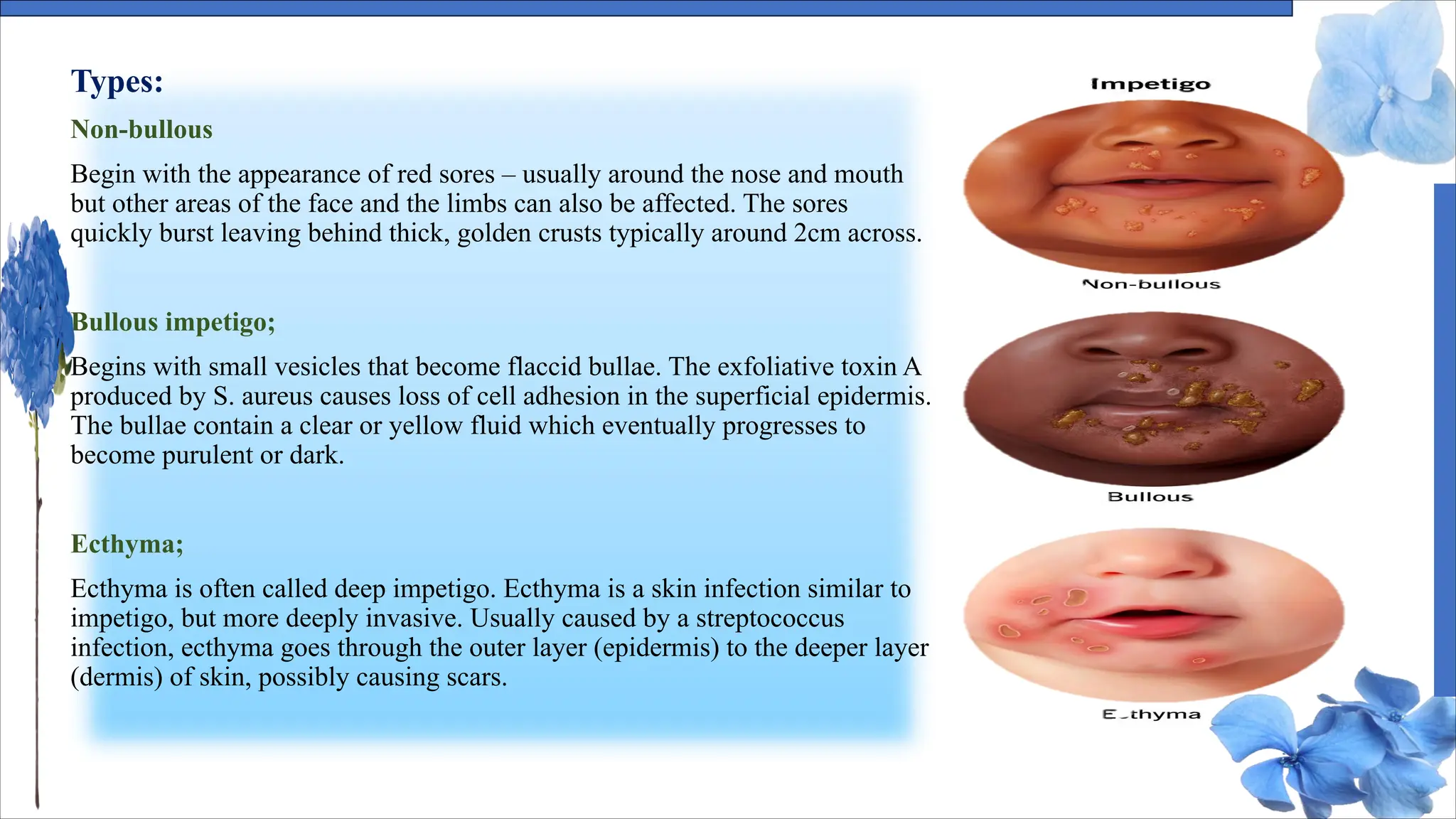
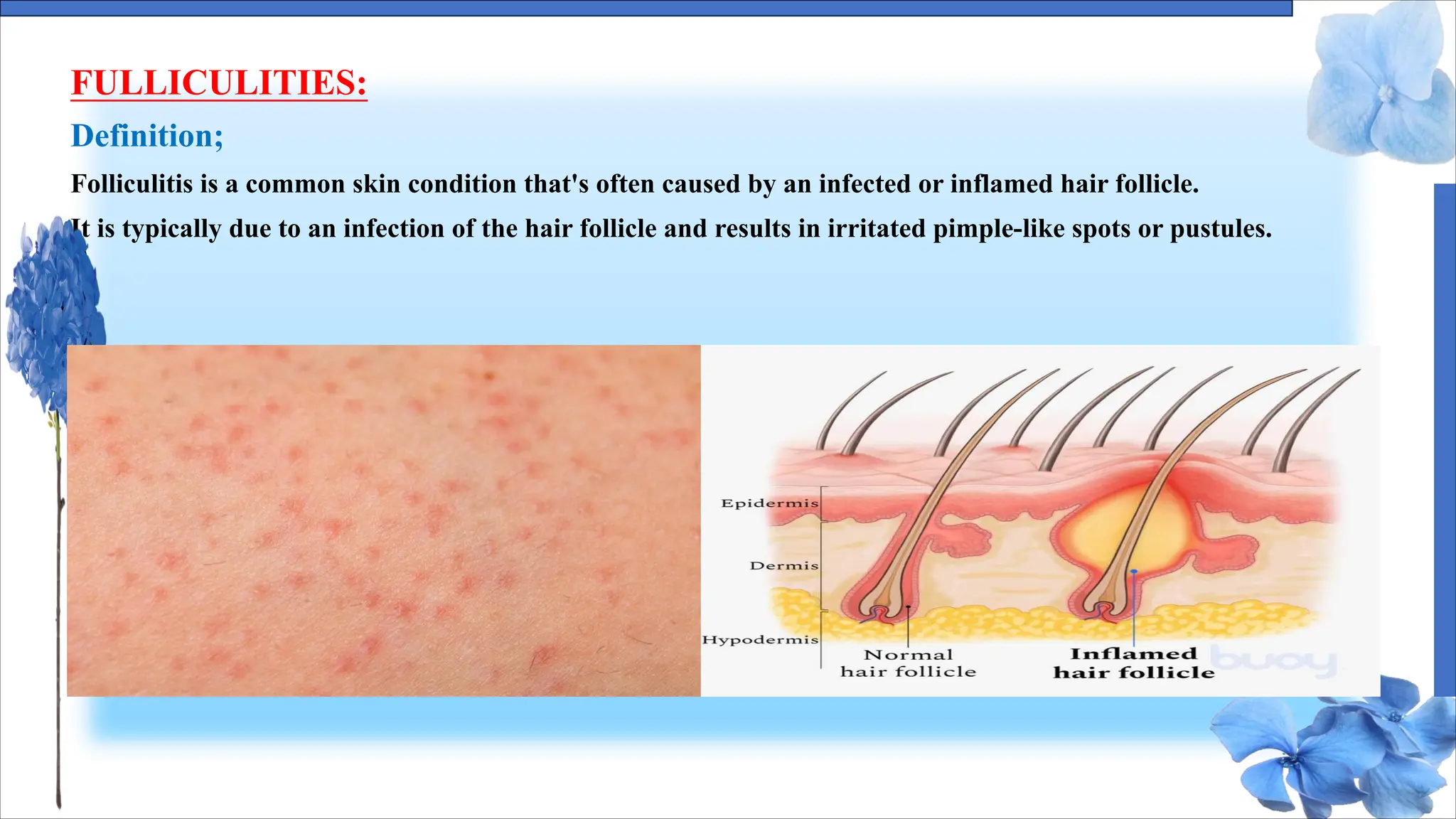
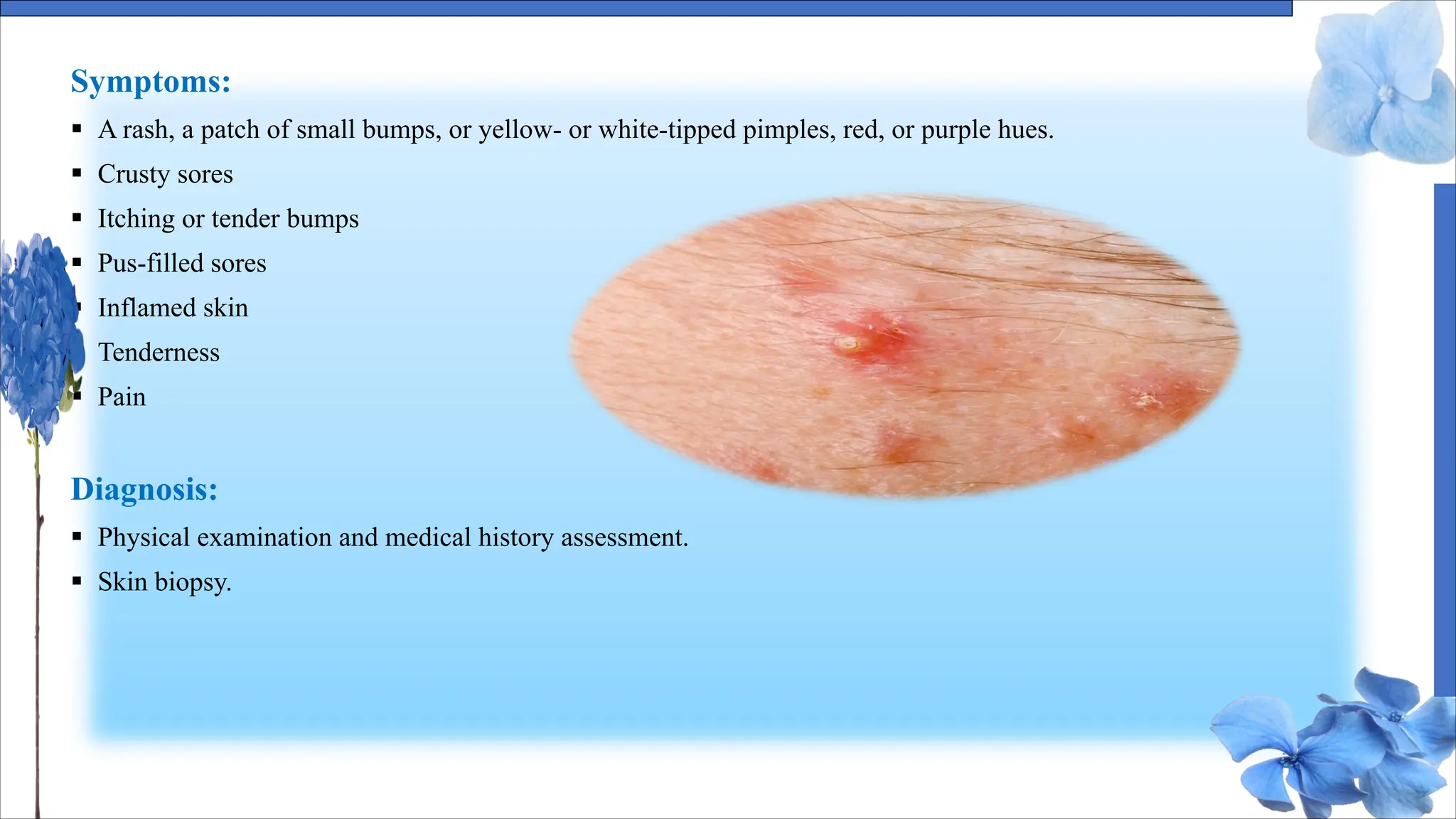

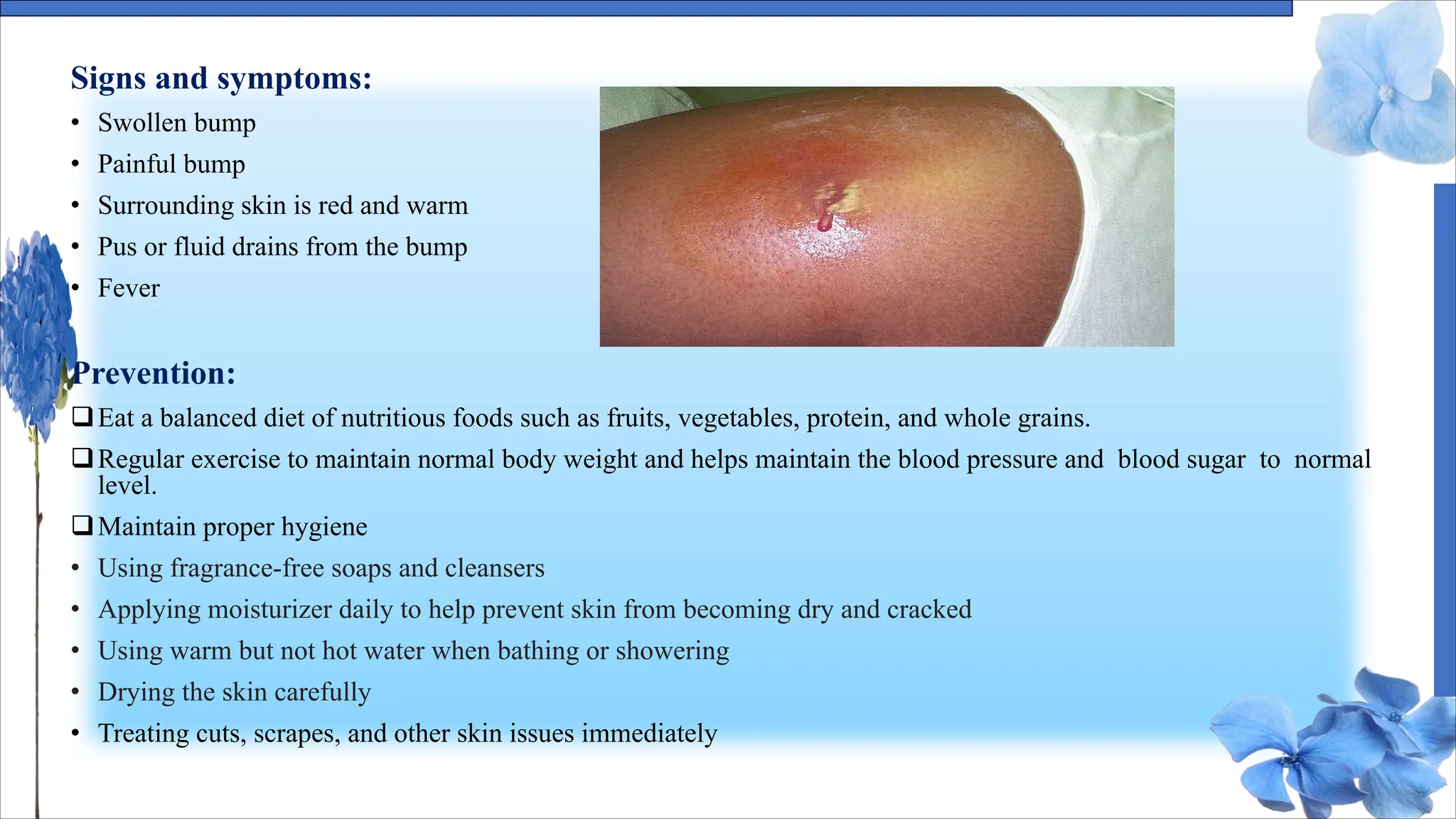
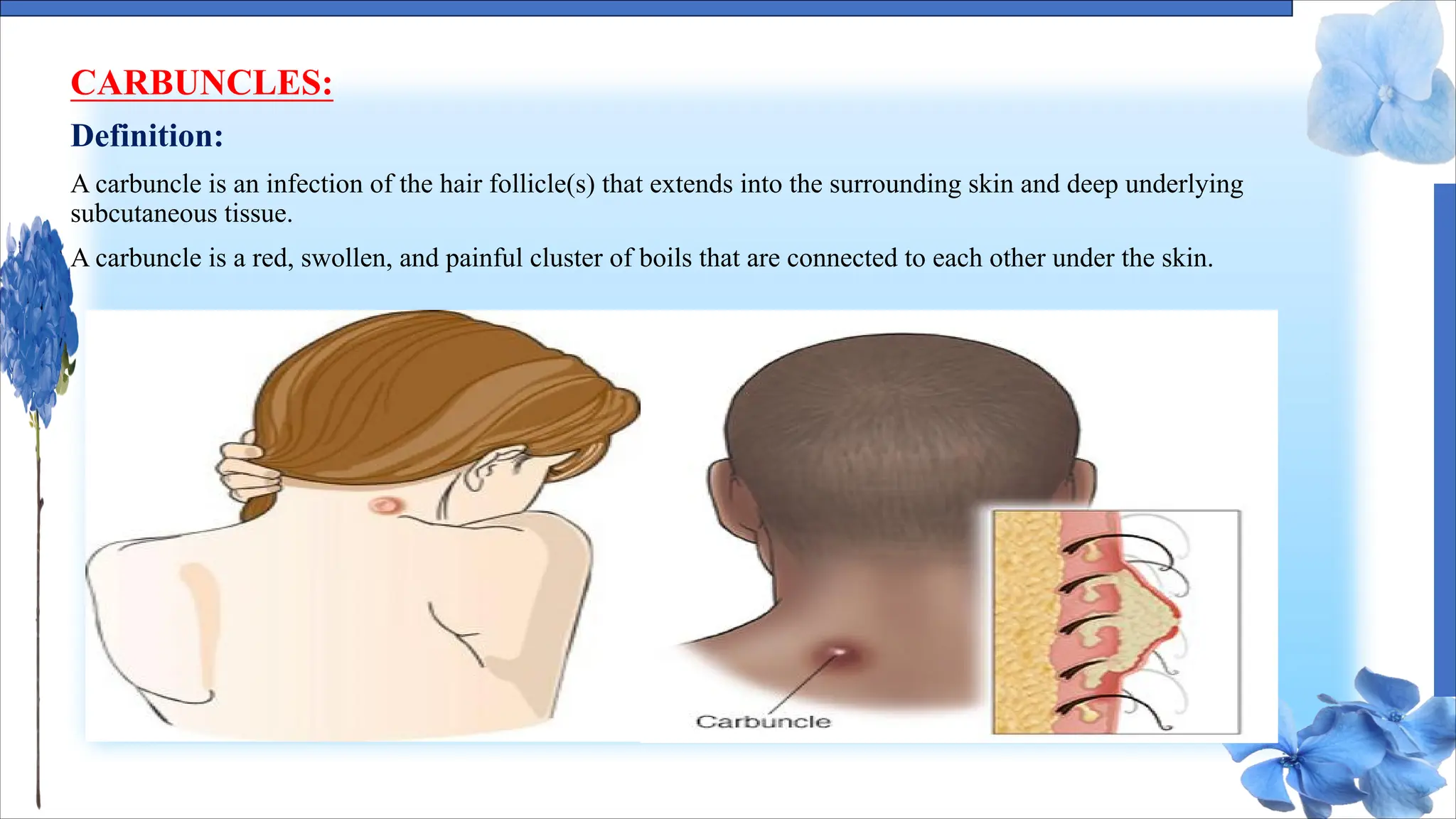
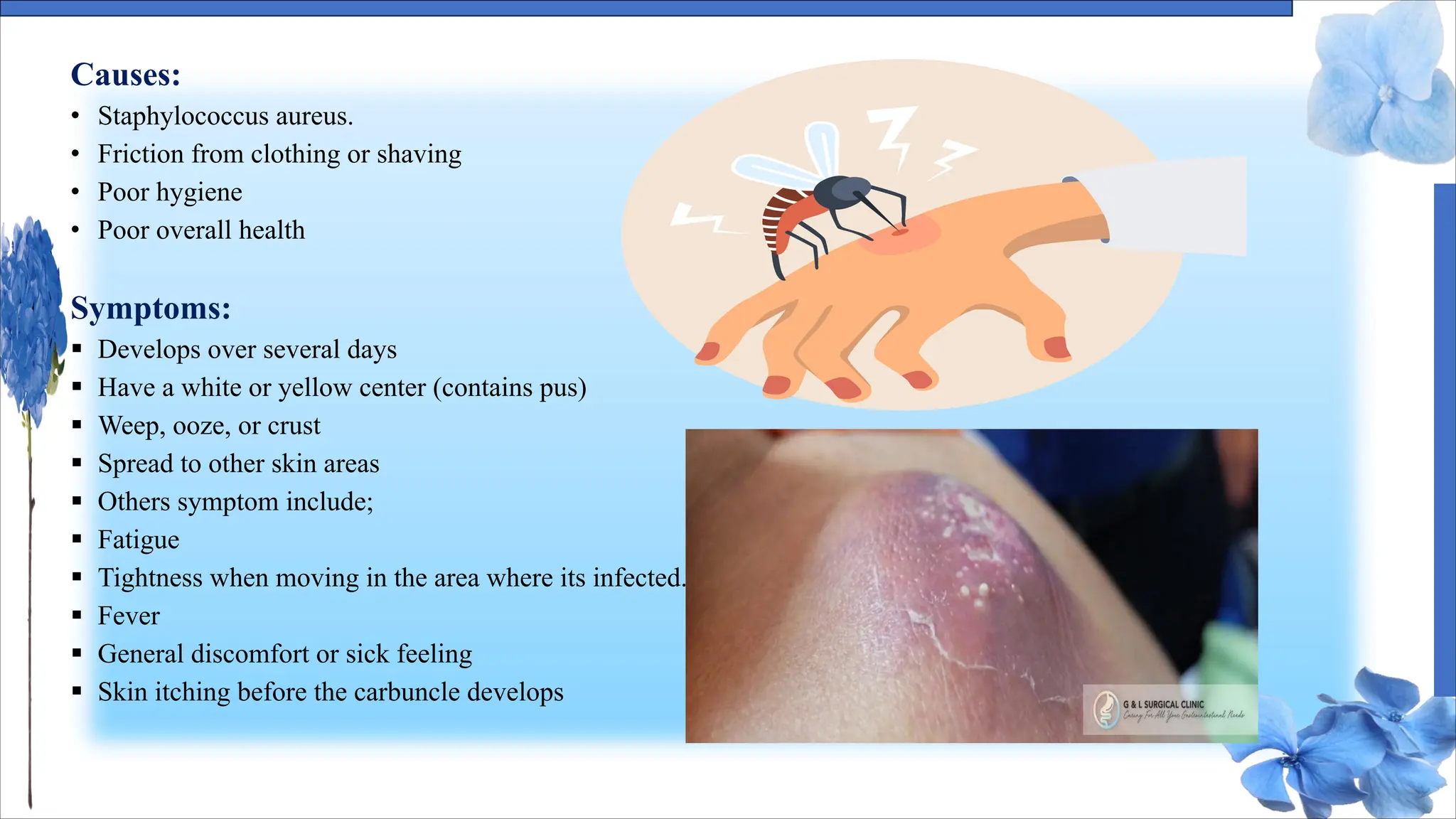


The document discusses various skin conditions including pyoderma, impetigo, folliculitis, furuncles, and carbuncles, detailing their definitions, causes, symptoms, diagnosis, and management strategies. Pyoderma gangrenosum causes painful ulcers, while impetigo is a contagious infection characterized by sores. Other conditions such as folliculitis and furuncles are associated with infected hair follicles, with specific treatments ranging from antibiotics to lifestyle changes.























































































