Downloaded 33 times


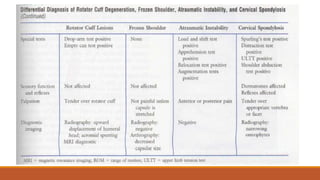


The document provides a comprehensive overview of the shoulder complex, detailing its anatomical components including the shoulder girdle, joints, and ligaments that contribute to its function and stability. It also discusses the motions available at the shoulder, the significance of the rotator cuff, and various assessment techniques to evaluate shoulder conditions, particularly in relation to injuries and age-related changes. The text emphasizes the importance of understanding the dynamic interactions of the muscles and ligaments for maintaining shoulder health and function.