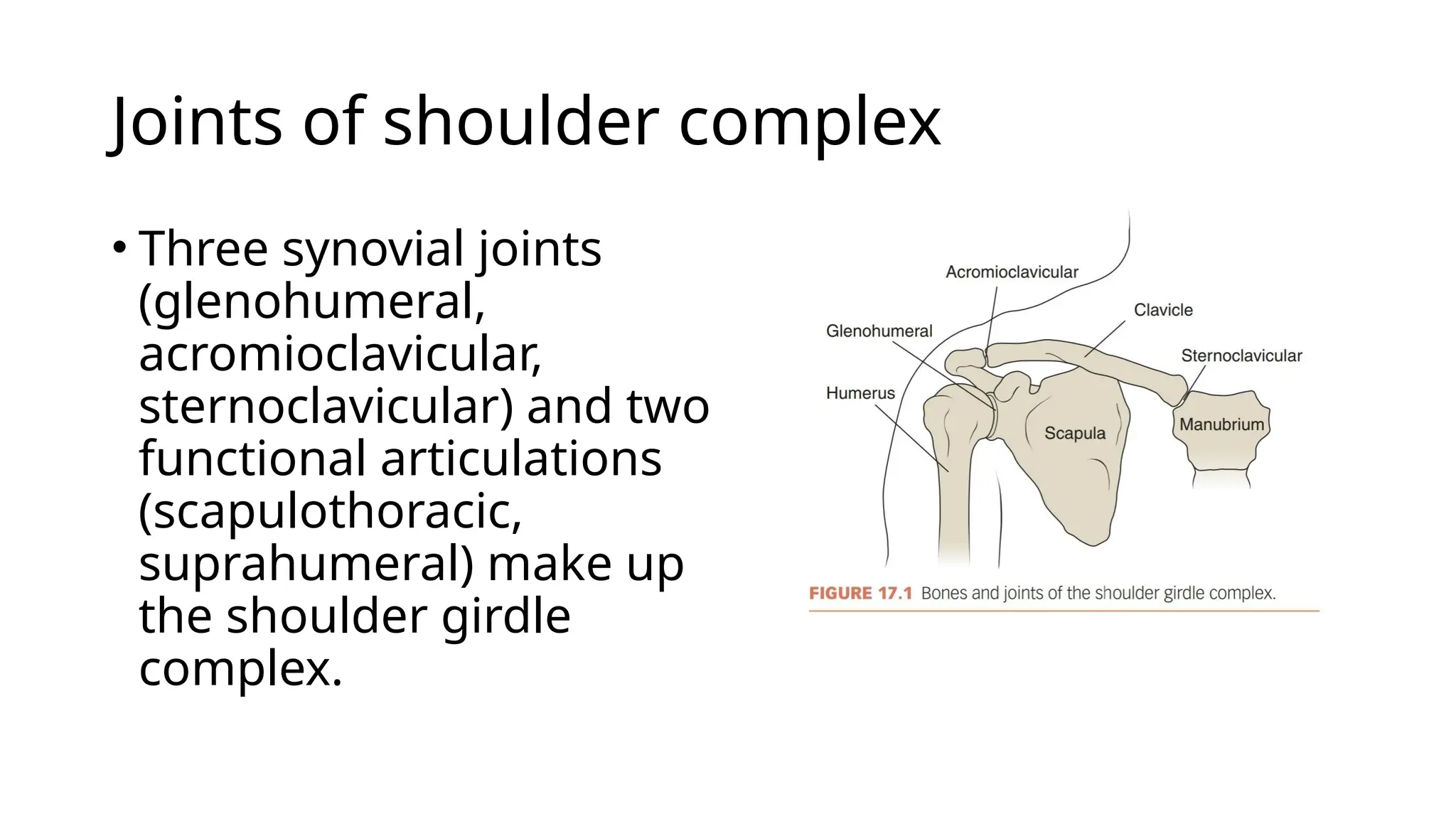
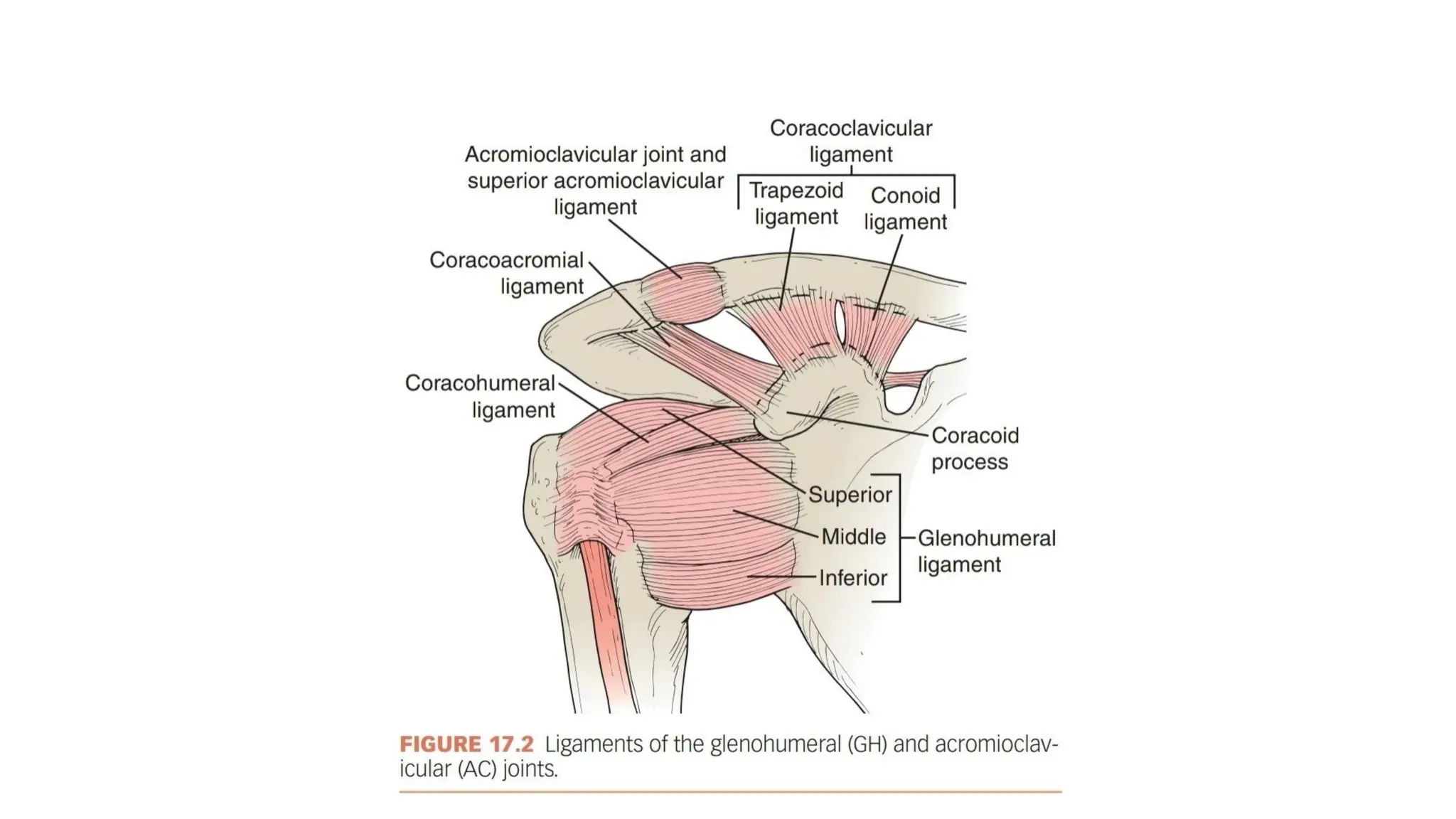
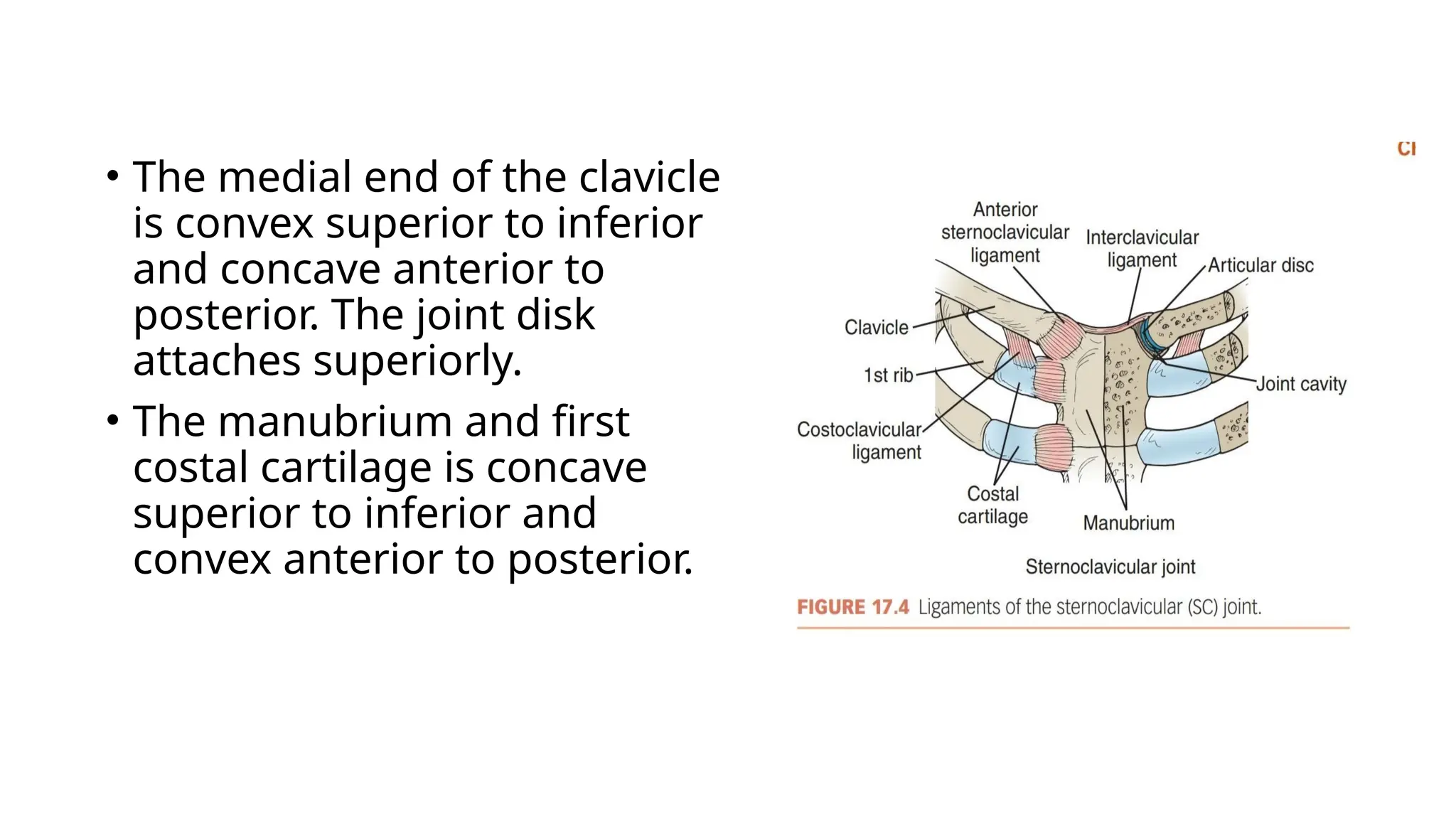
The document provides an overview of the shoulder complex, detailing the anatomy and biomechanics of the joints involved, including the glenohumeral, sternoclavicular, and acromioclavicular joints. It explains key concepts such as the convex-concave rule, scapulohumeral rhythm, and the roles of various muscles in stabilizing the shoulder during movement. Additionally, it discusses the importance of coordinated motions between the scapula and humerus to achieve full shoulder range of motion.