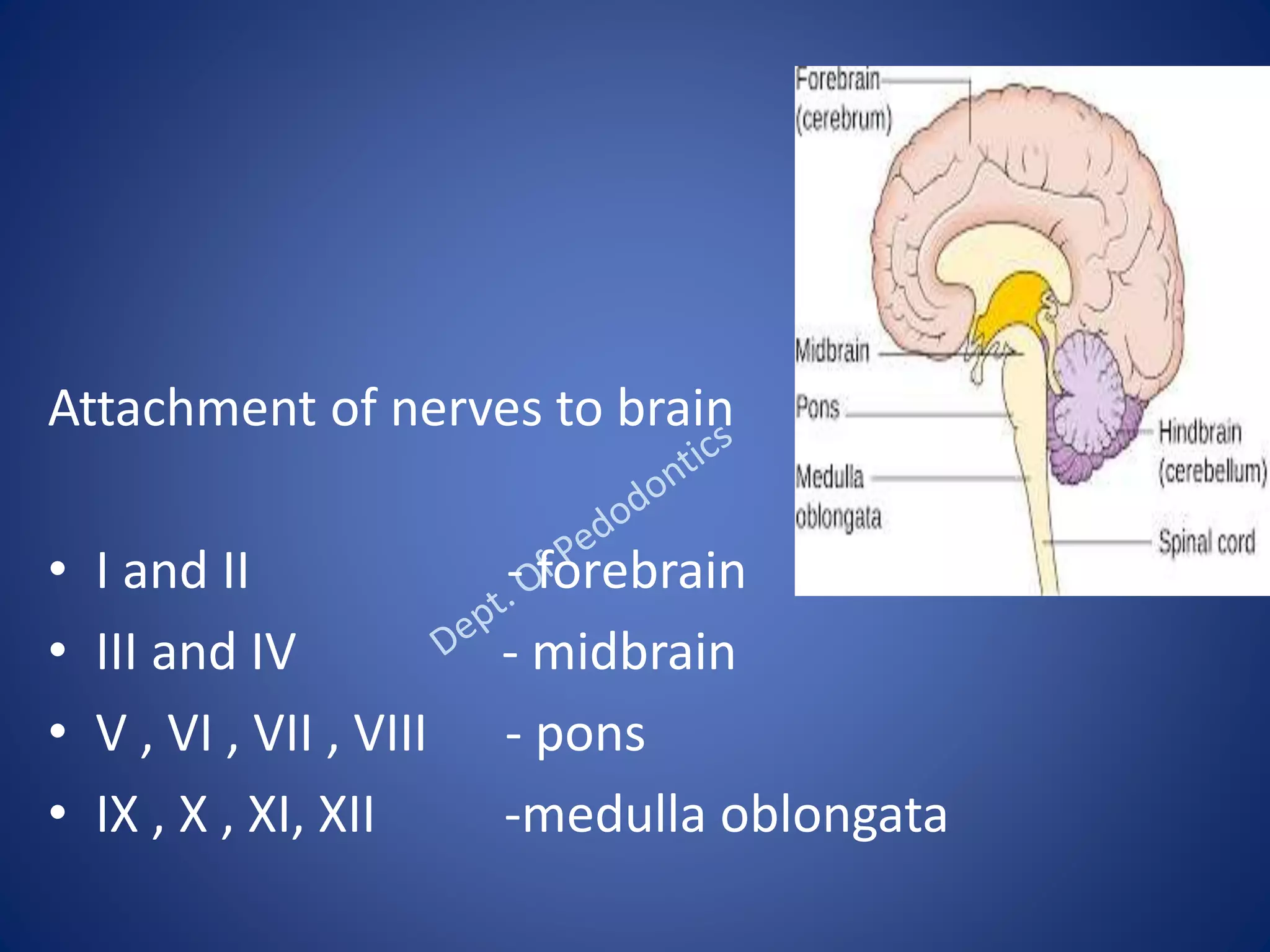
The document discusses the 12 pairs of cranial nerves. It provides detailed information on the olfactory, optic, oculomotor, trochlear, trigeminal, abducent, and facial cranial nerves. It describes the embryology, course, distribution and functions of these nerves. It also discusses various clinical conditions that can arise from injuries or lesions to the different cranial nerves.