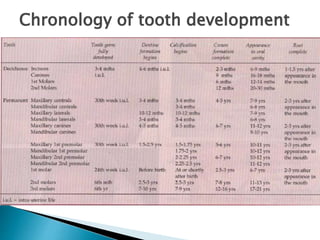
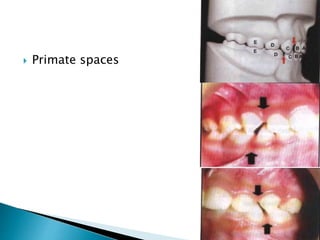
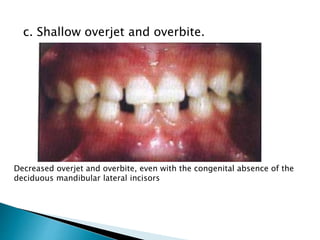
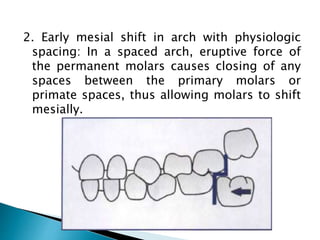
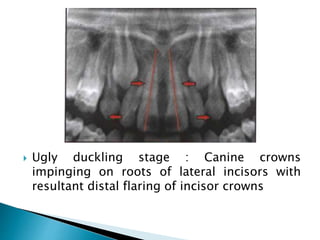
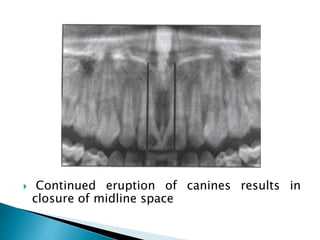
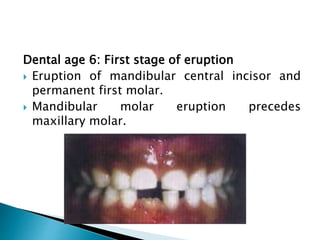
The document outlines the chronology of tooth development, detailing the formation and eruption of both primary and permanent teeth, starting from gum pads at birth to the establishment of the permanent dentition by age 13. It describes various stages of tooth development, including pre-eruptive, eruptive, and post-eruptive movements, as well as specific features such as spacing, molar relationships, and the phenomenon of the 'ugly duckling stage' during dental changes. The document emphasizes the importance of dental age, eruptive sequences, and changes in jaw size and alignment throughout early childhood to early adolescence.