



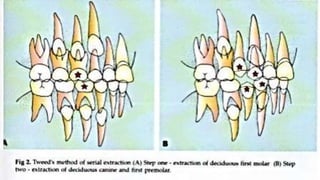
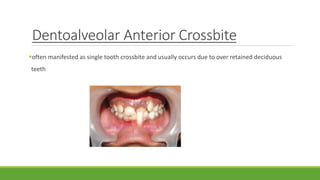




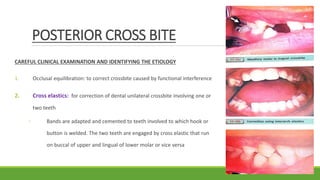








Interceptive orthodontics refers to early orthodontic treatment during mixed dentition to guide proper development of the dentition. Common procedures include serial extraction to relieve crowding, correction of developing crossbites, and control of abnormal habits like thumb sucking. Early intervention is beneficial as it is simpler and more stable than later treatment, prevents worsening of issues, and offers psychological benefits to children. The optimal age for screening and interceptive treatment is around 9-11 years old.














































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



