Download as PDF, PPTX
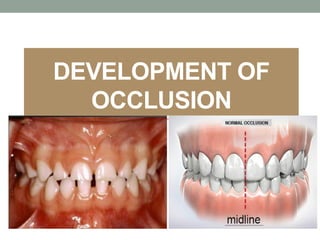















































This document discusses the development of occlusion from the neonatal period through adulthood. It covers the following key points: 1. Occlusion develops through four periods: neonatal, primary dentition, mixed dentition, and permanent dentition. Each period has characteristic features and relationships between the teeth. 2. During the neonatal period, the gum pads have an anterior open bite relationship. As the primary teeth erupt, different molar relationships can form that influence the permanent dentition. 3. In the mixed dentition period, the first permanent molars erupt and can cause early or late shifts to a class I molar relationship through mechanisms like leeway space. Anterior teeth are also exchanged.