Downloaded 22 times

























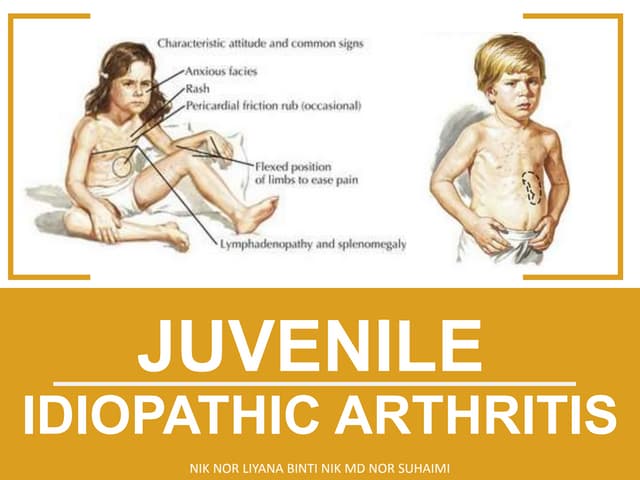
Juvenile idiopathic arthritis (JIA) is a chronic form of arthritis in children under 16 years old that lasts over 6 weeks. The cause is unknown but believed to be autoimmune. There are several subtypes characterized by the number and type of joints involved and presence of systemic symptoms. Symptoms include joint swelling, pain, and stiffness. If untreated, JIA can cause joint damage and limited mobility. Treatment involves medications like NSAIDs, steroids, DMARDs, and biologics to reduce inflammation and prevent long-term issues. The goals are eliminating active disease, improving joint function, and allowing normal growth and development.