Downloaded 19 times
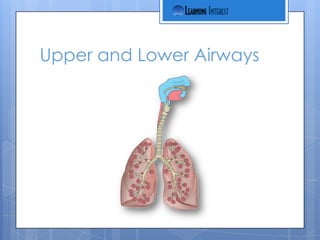

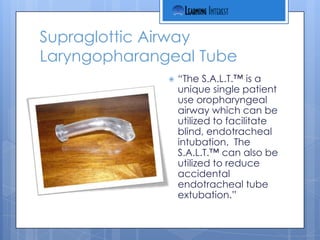
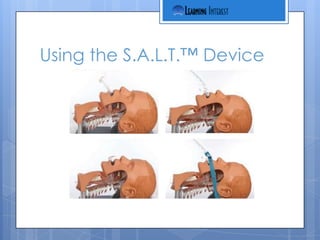

This document provides an overview and objectives for a training on anatomy of the upper and lower airways, ventilation, respiration, and use of the S.A.L.T.TM device. It describes the S.A.L.T.TM as a single-use oropharyngeal airway that can facilitate blind intubation and reduce accidental extubation. It also lists the standing medical order for use of the S.A.L.T.TM device, which allows its use after two unsuccessful intubation attempts to help guide placement of an endotracheal tube.