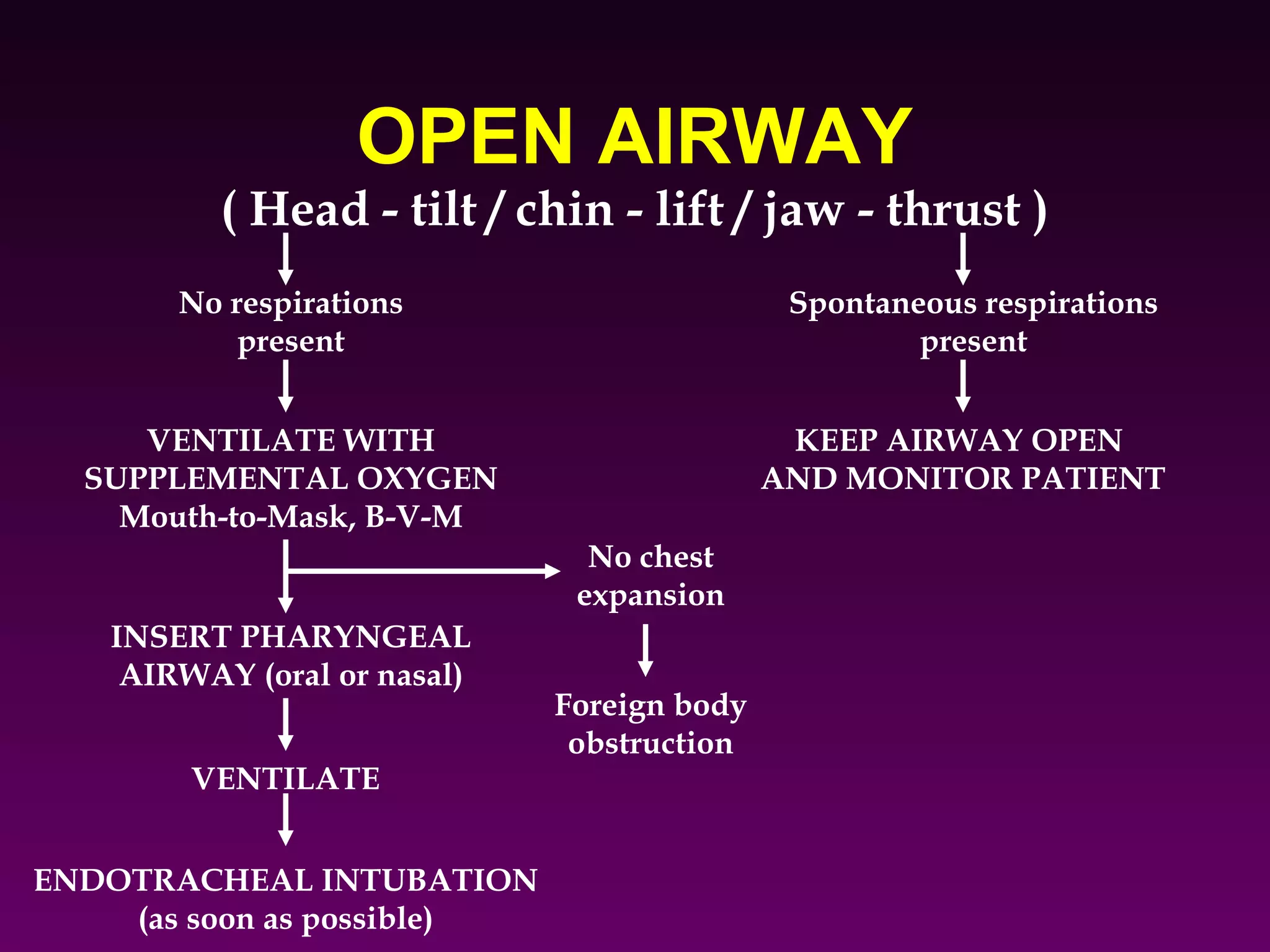
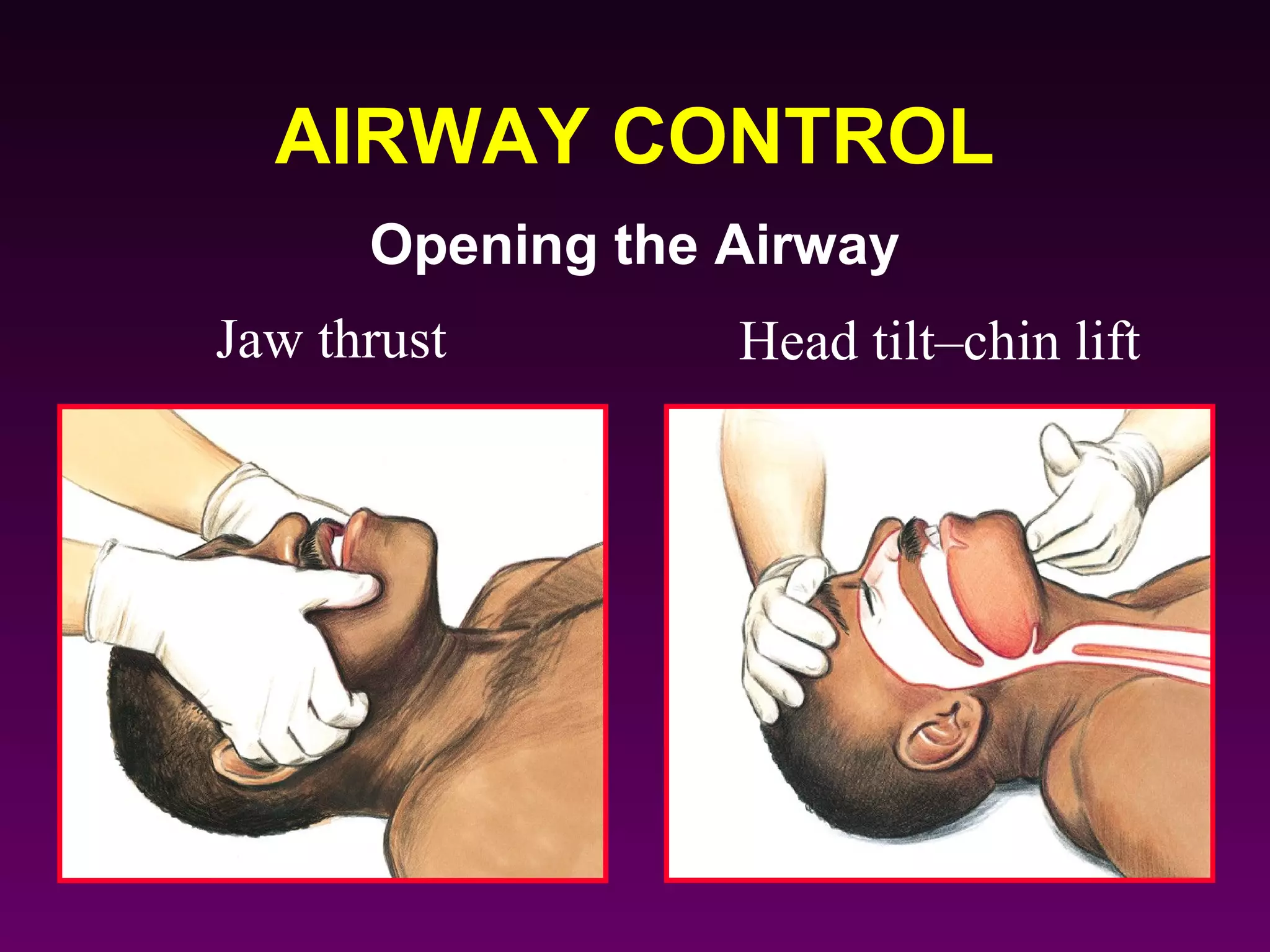
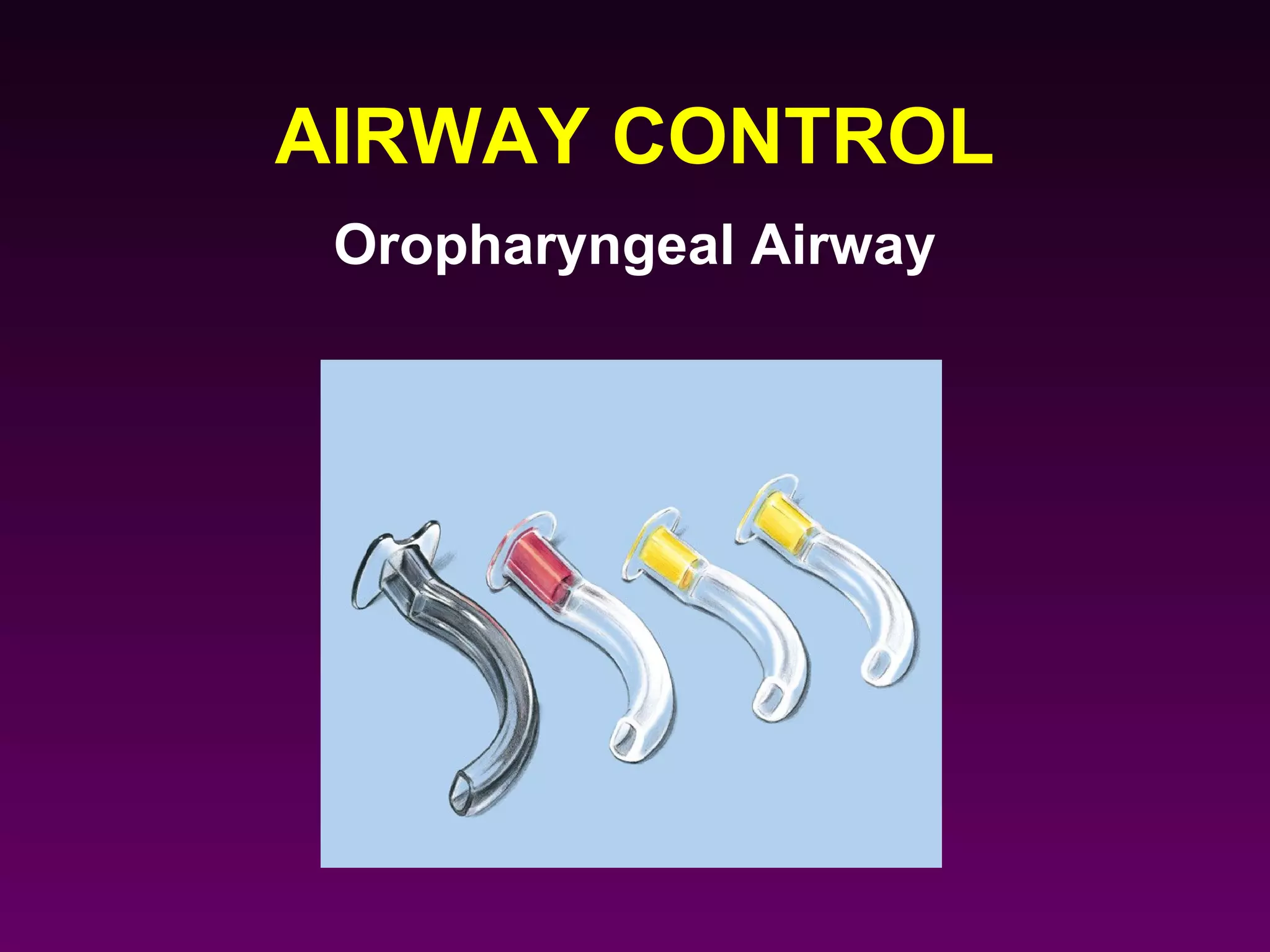
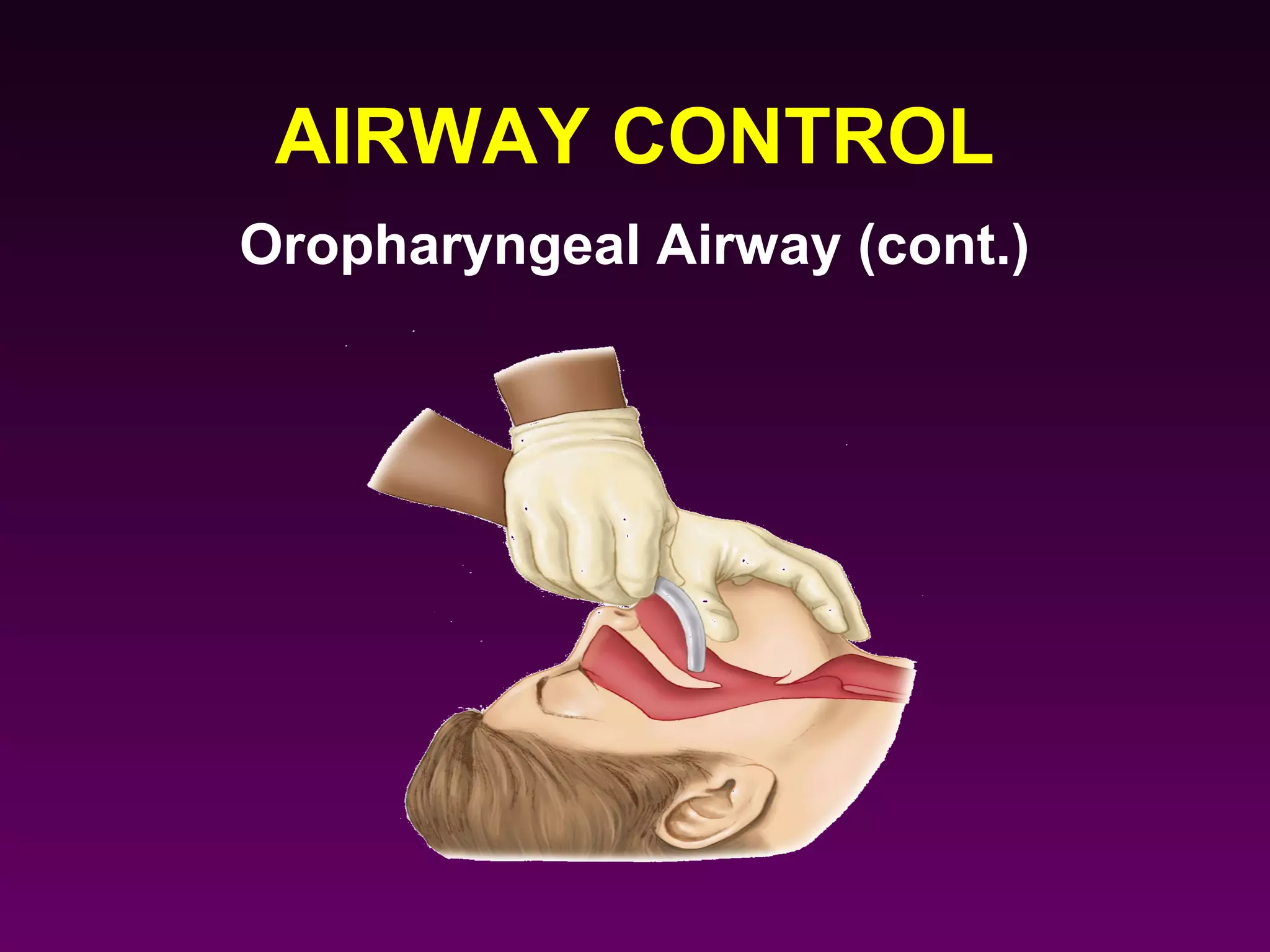
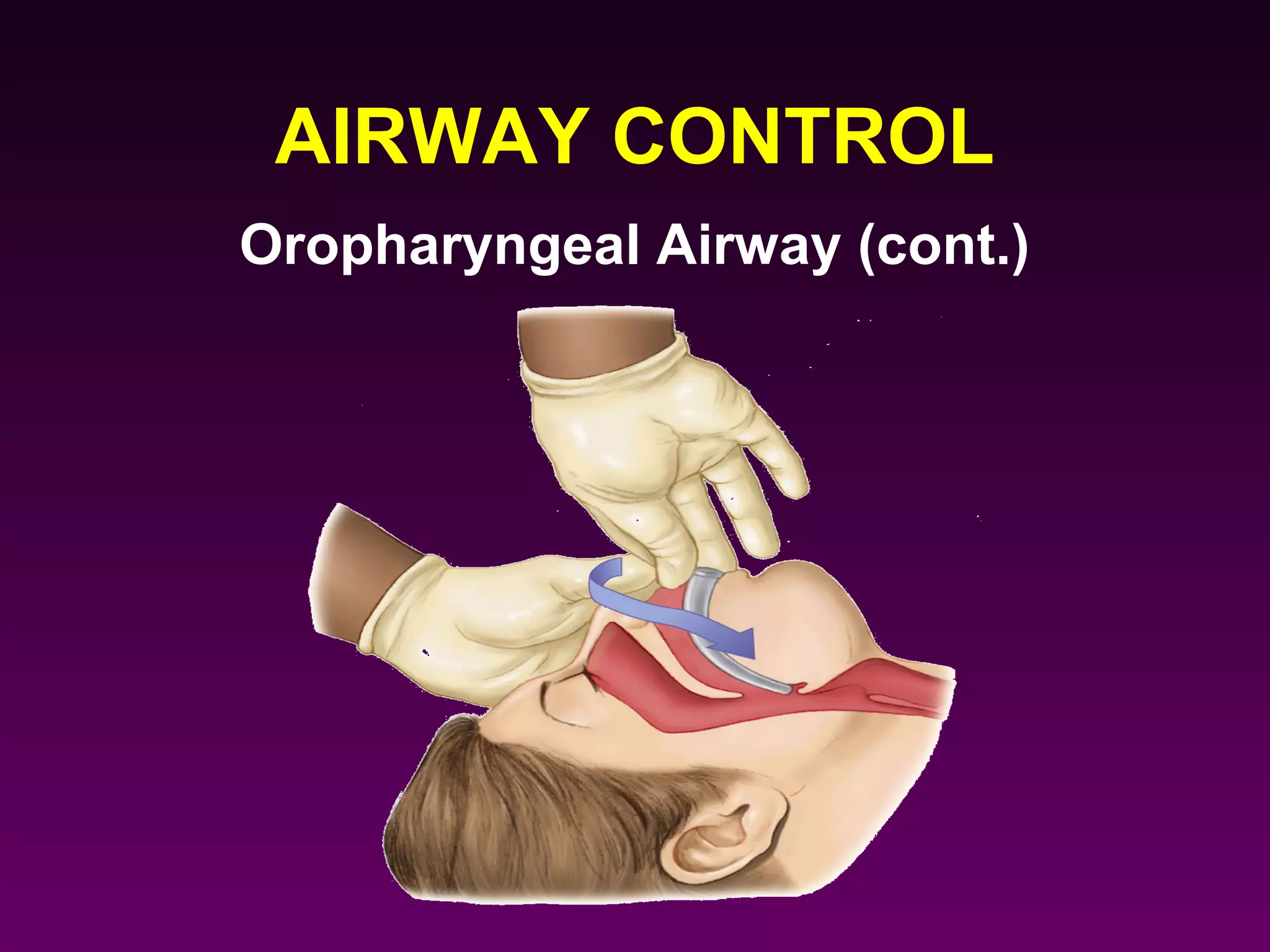
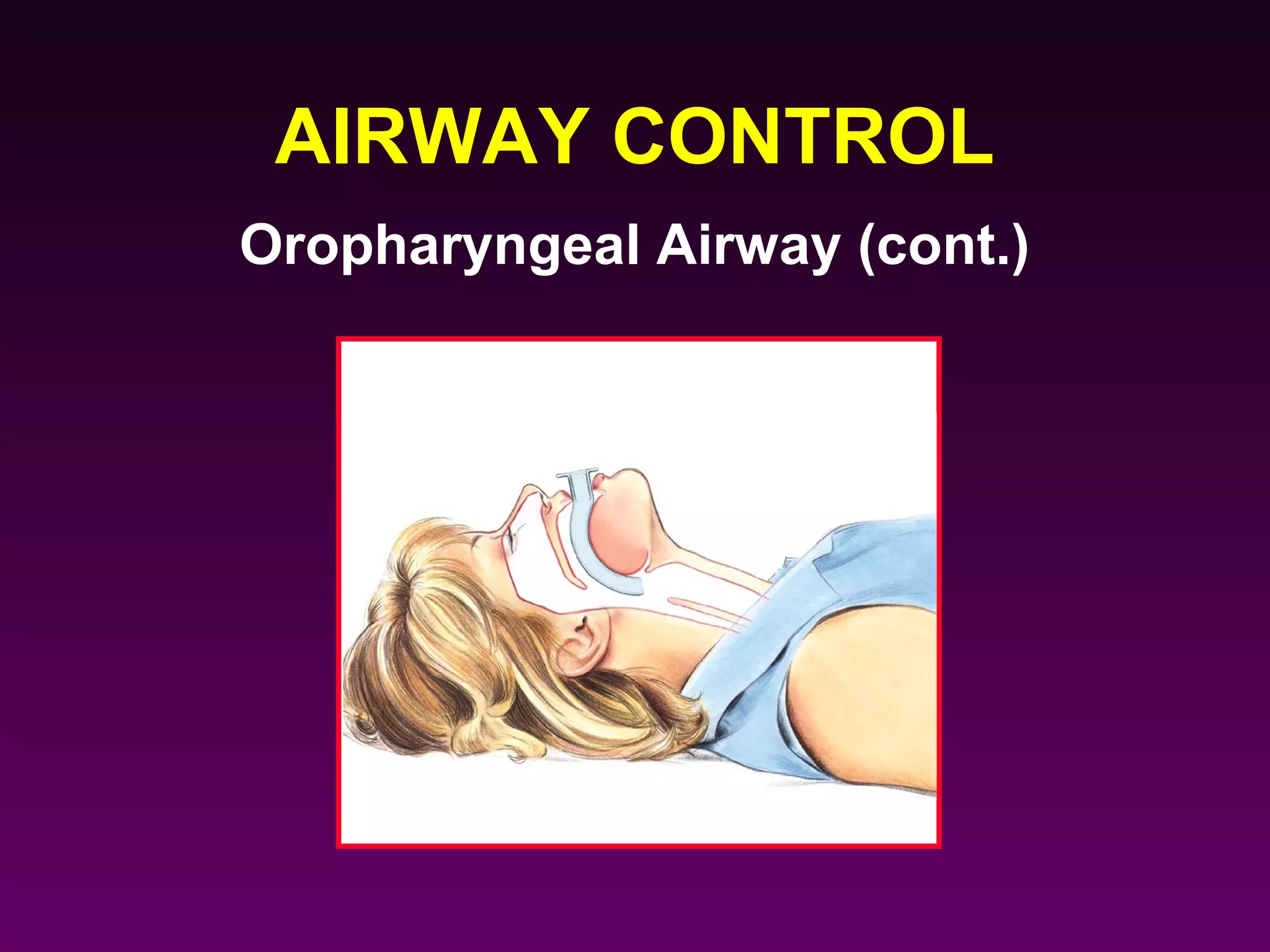
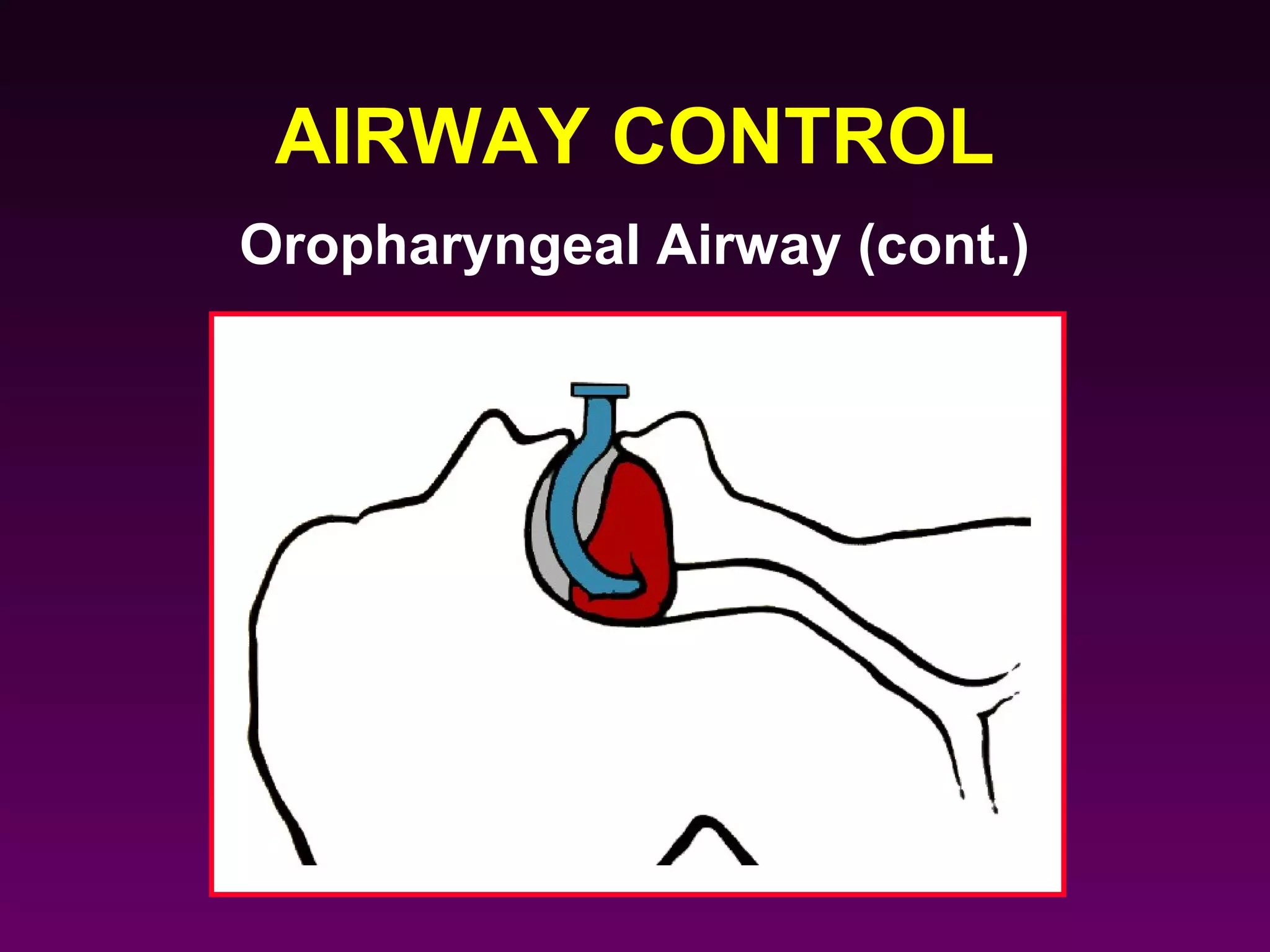
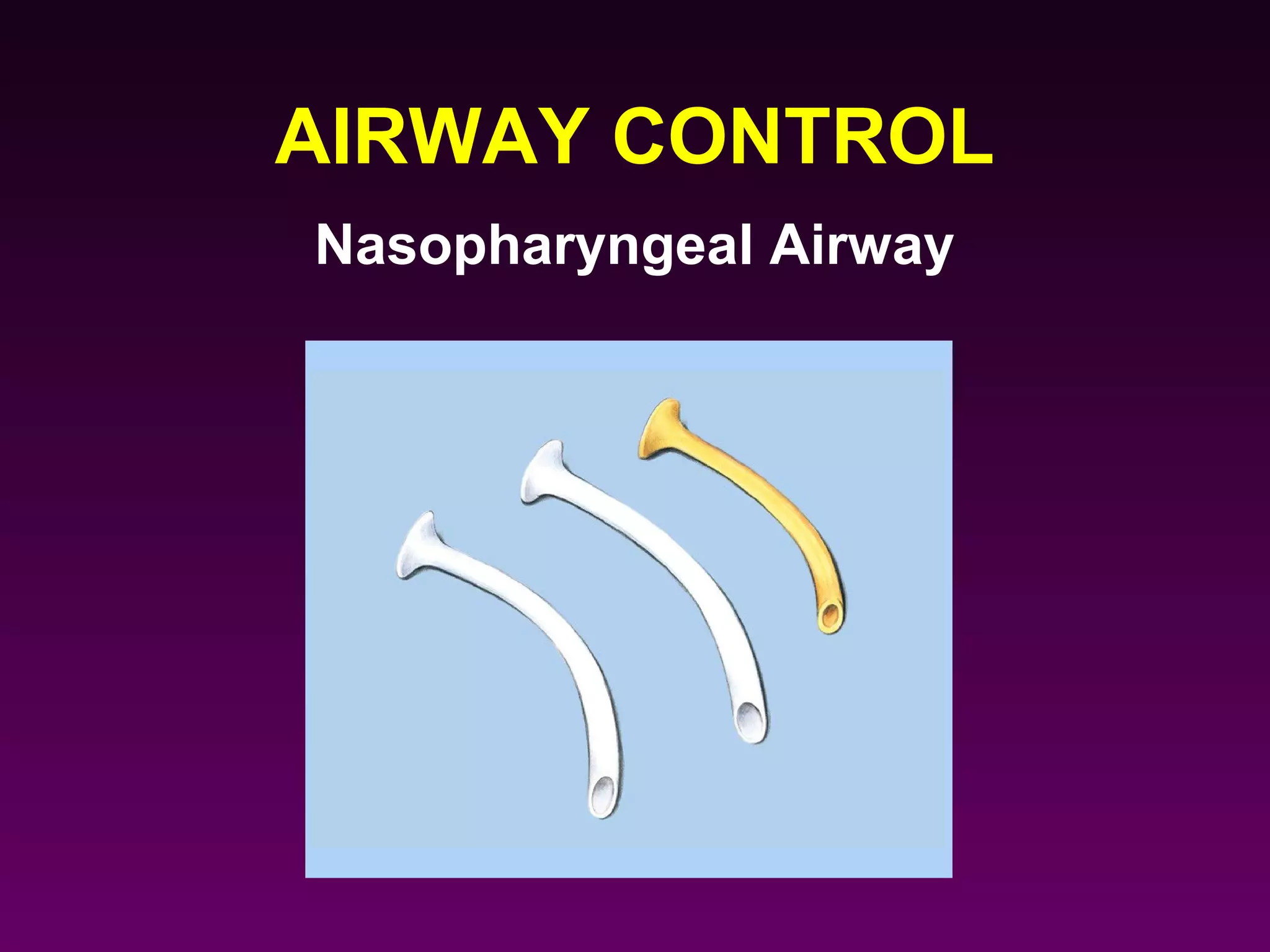
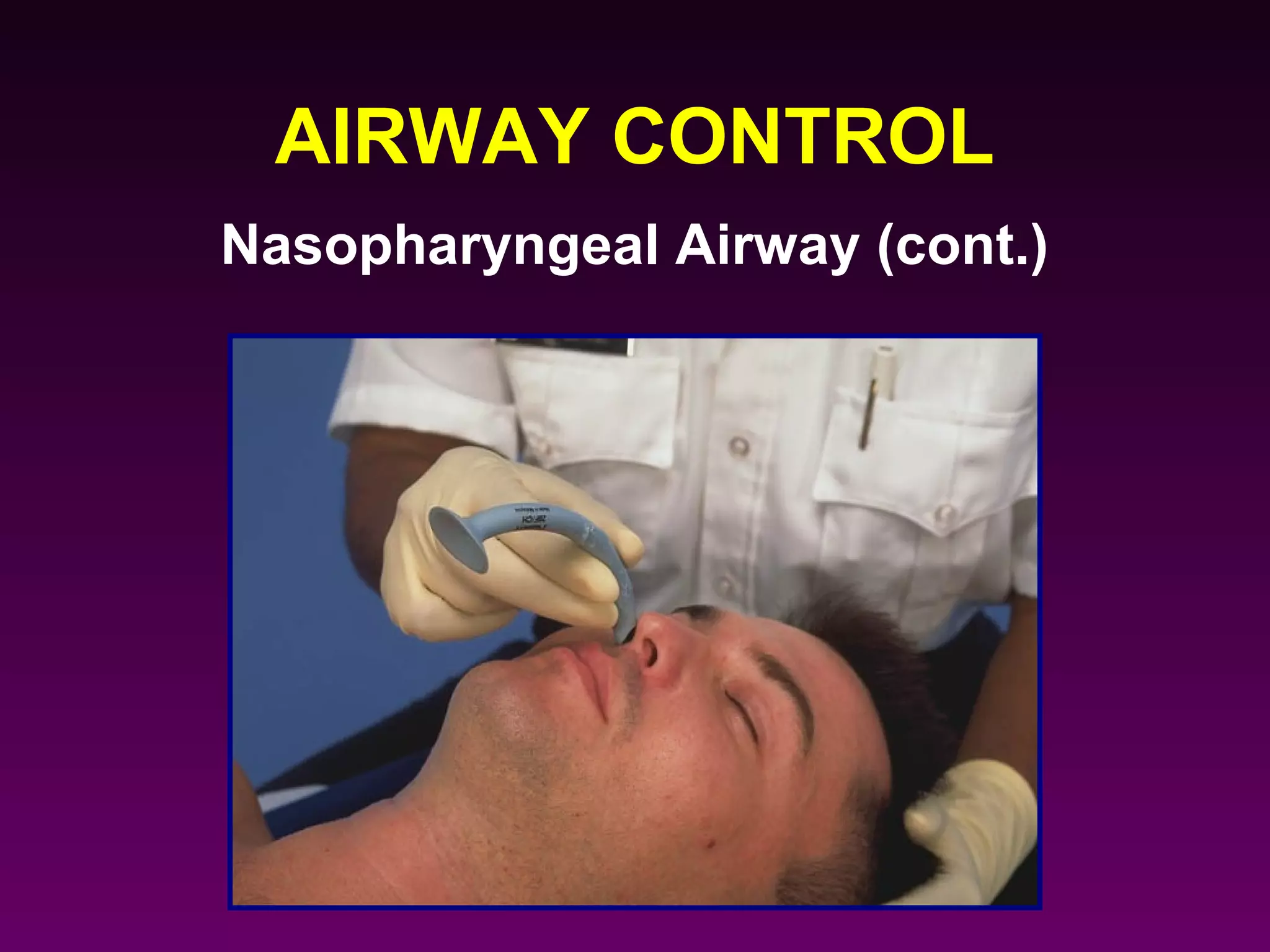
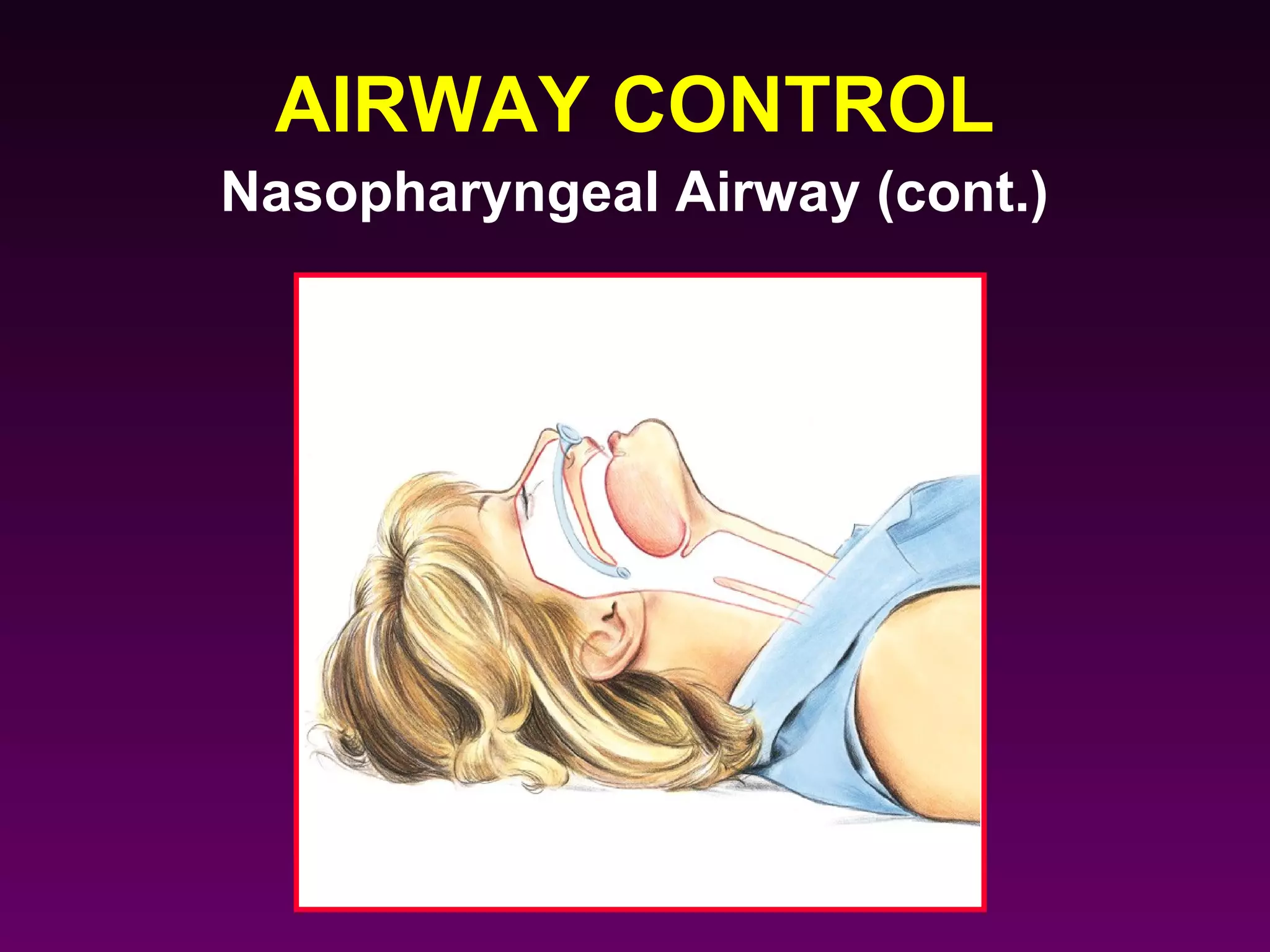
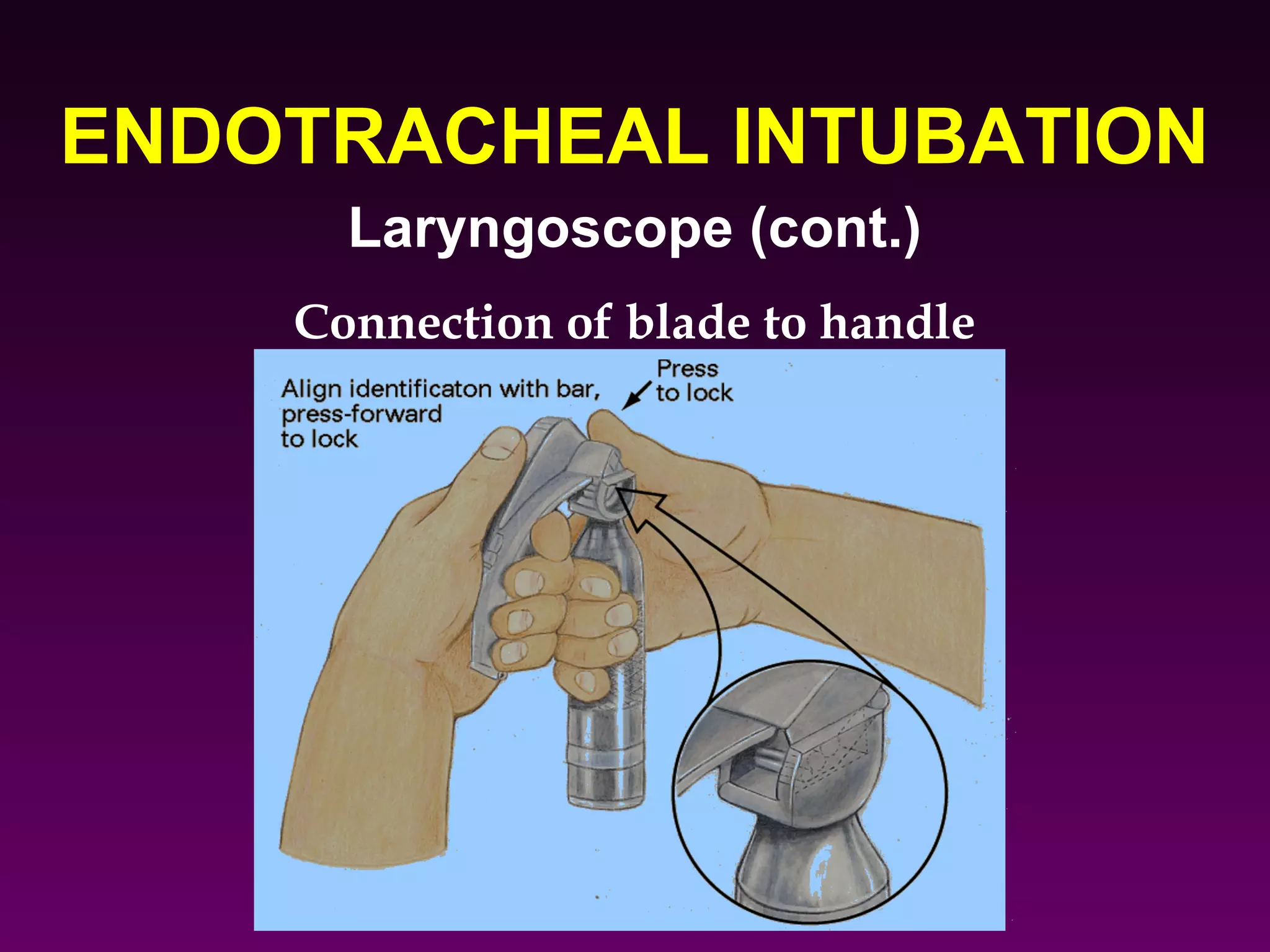
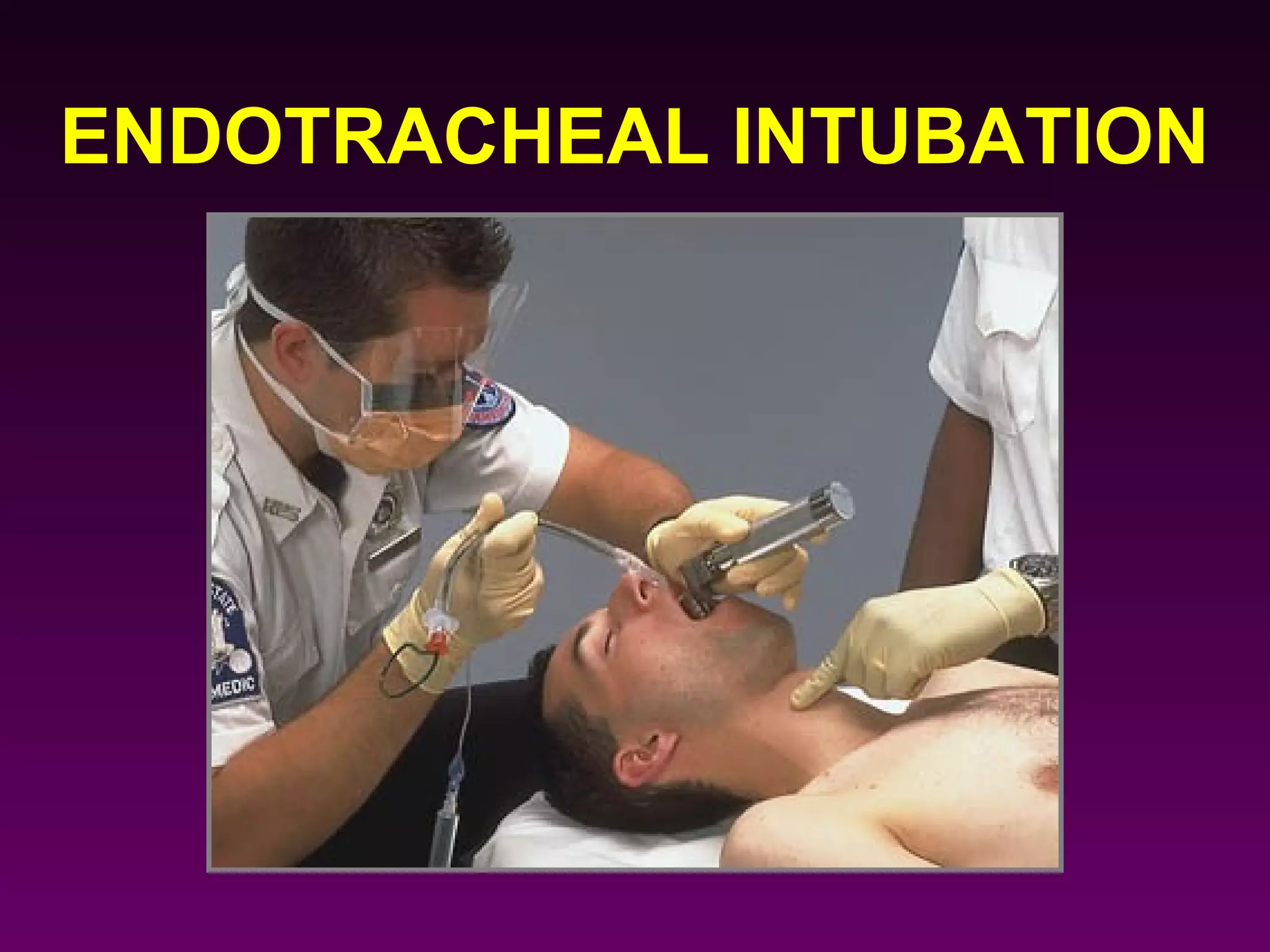
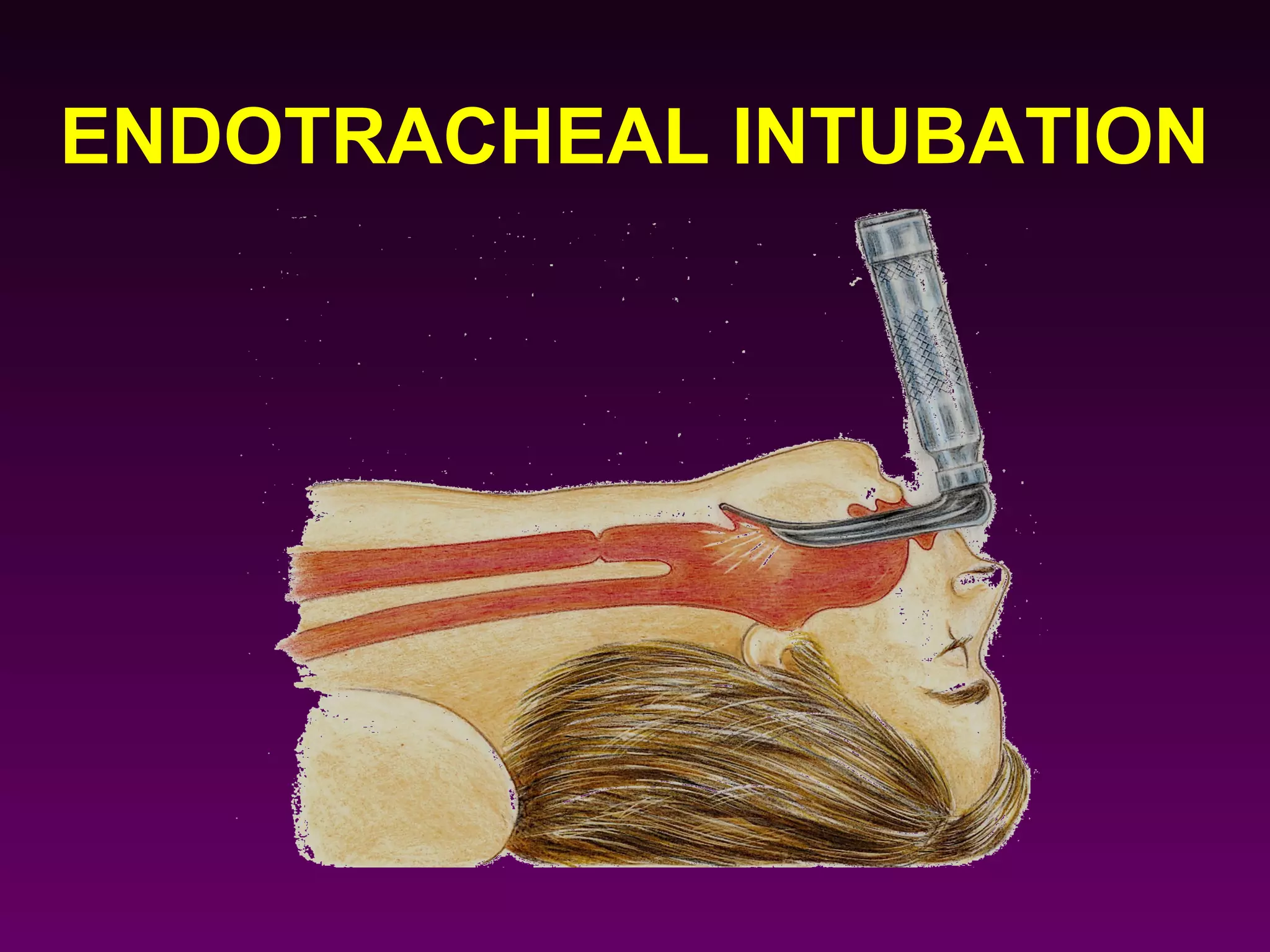
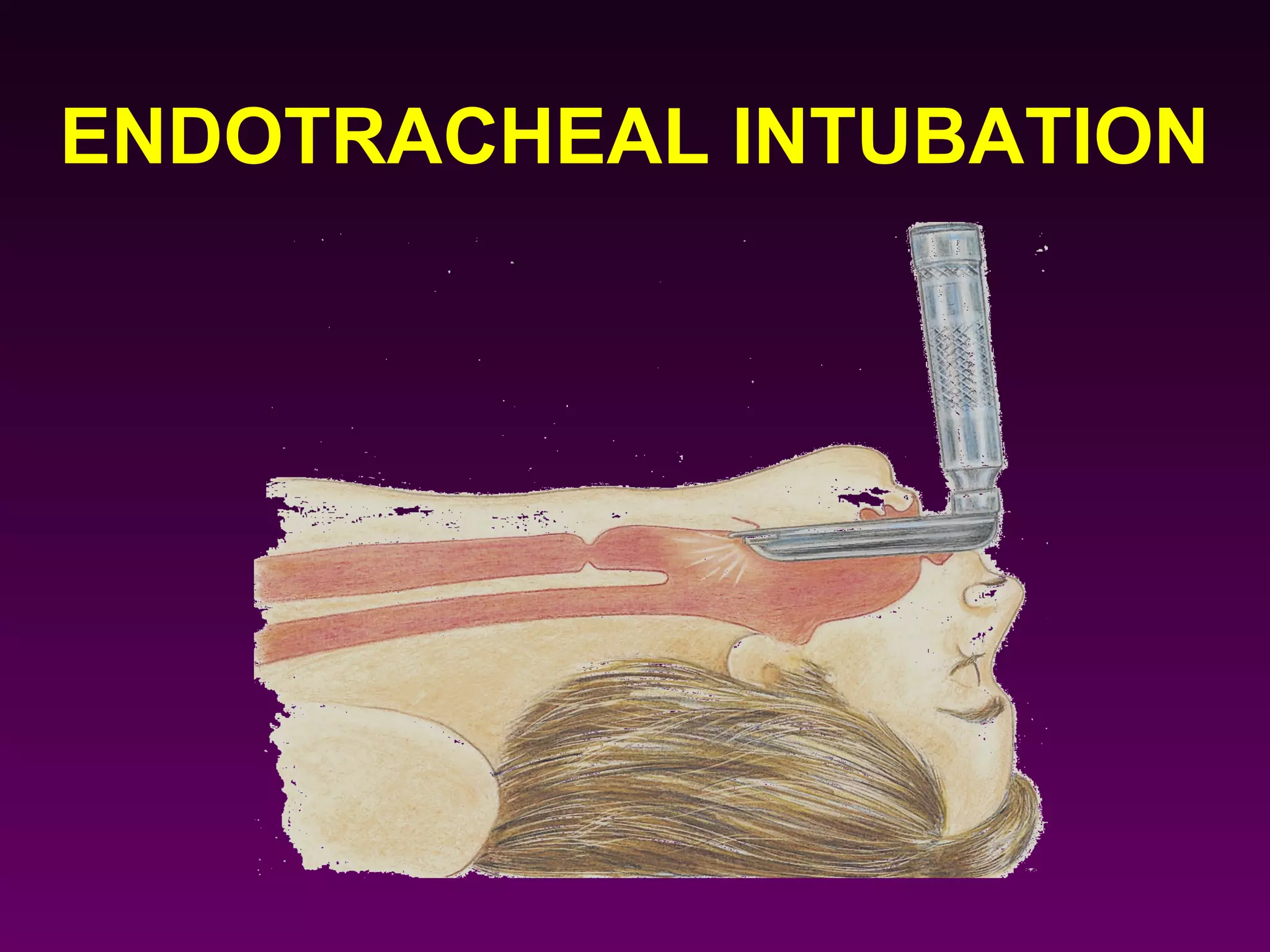
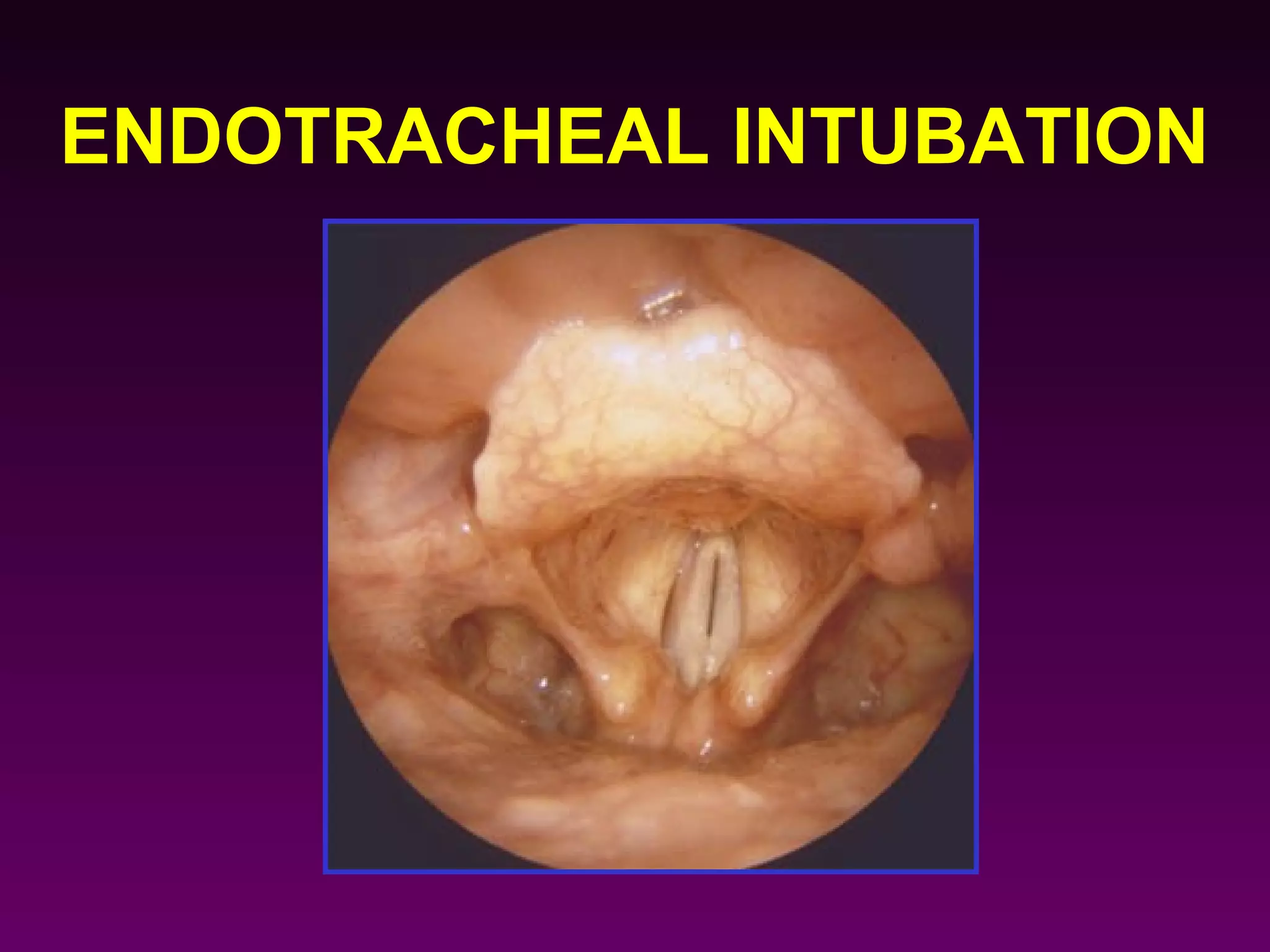
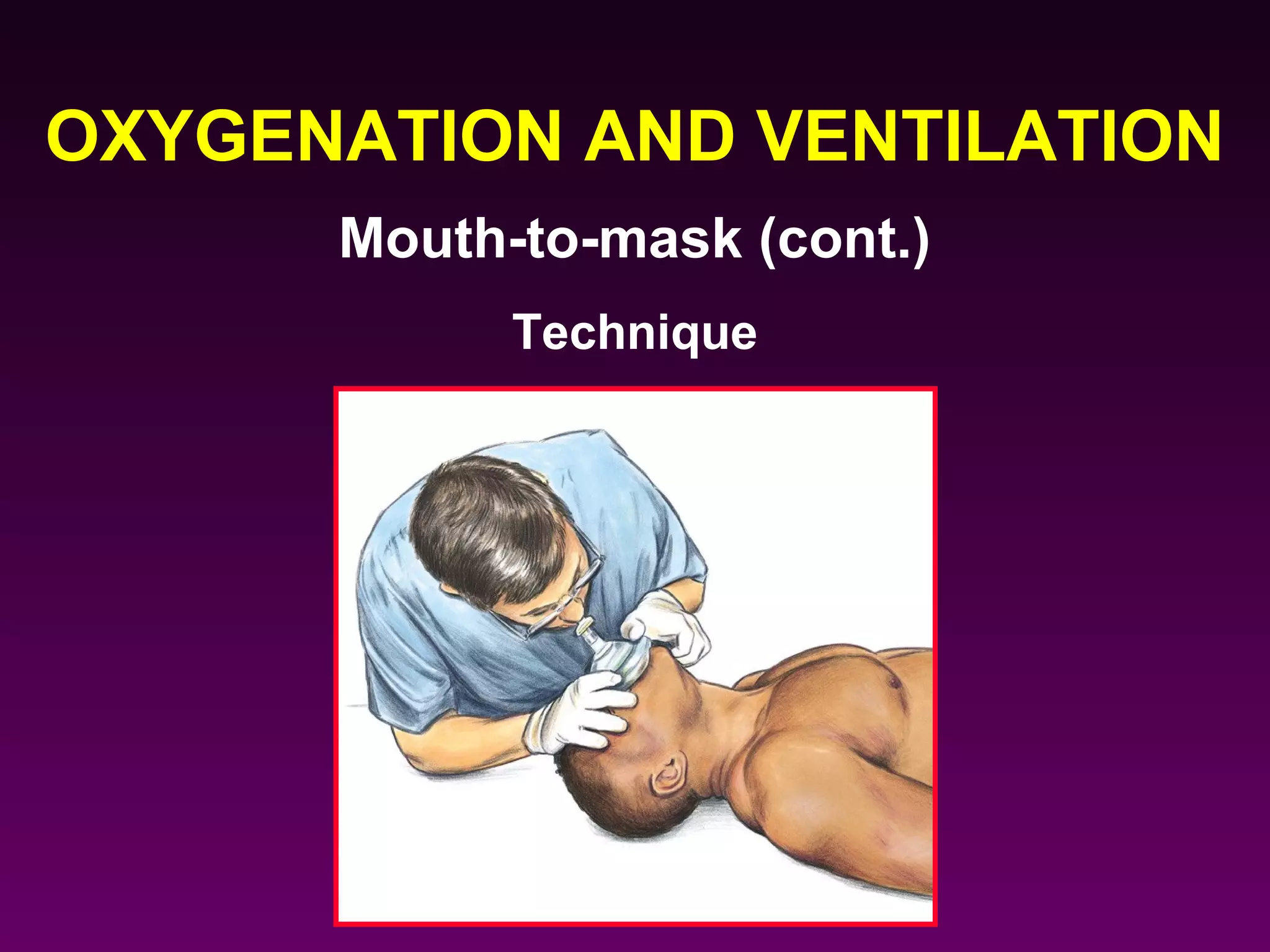
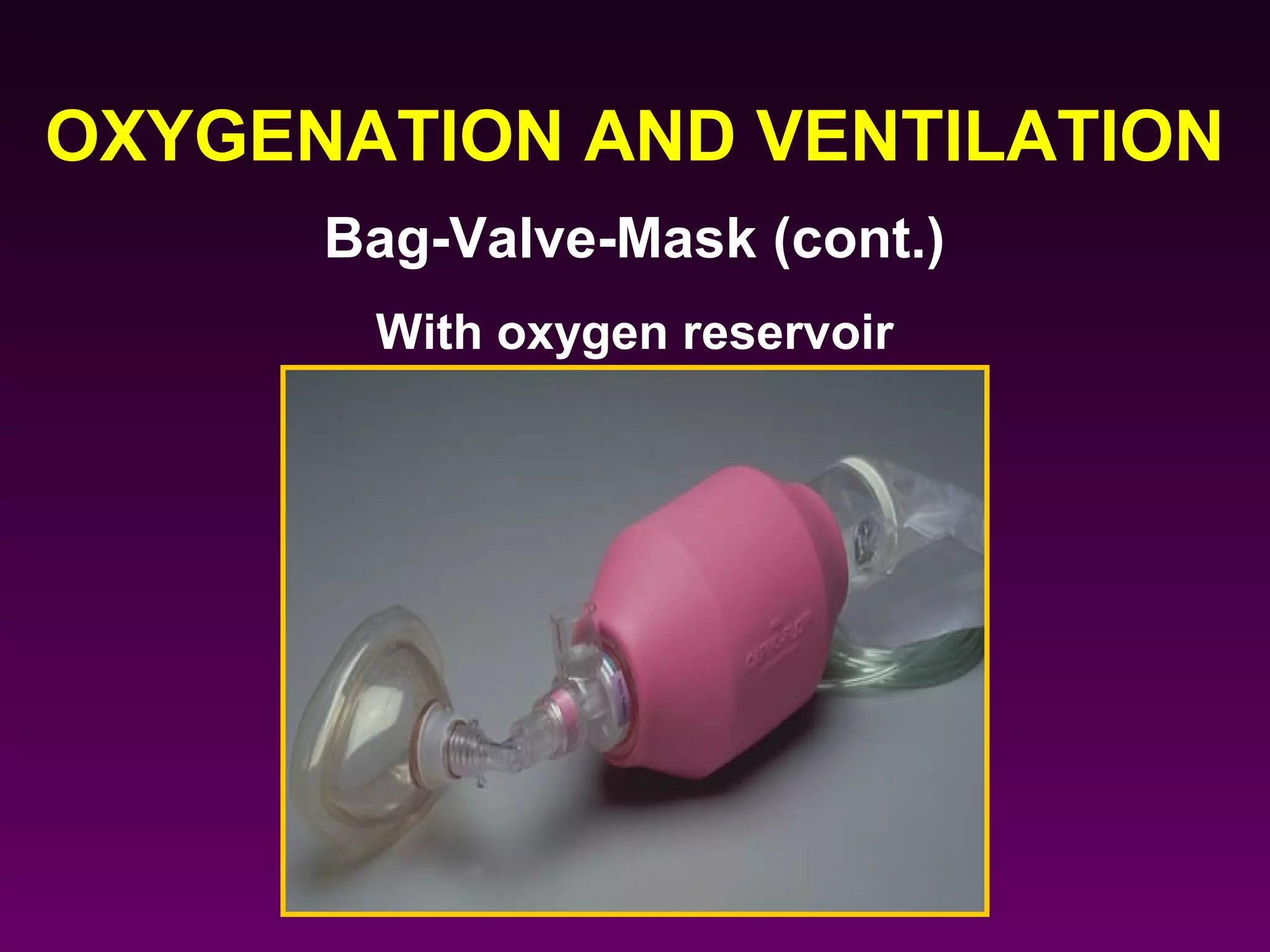
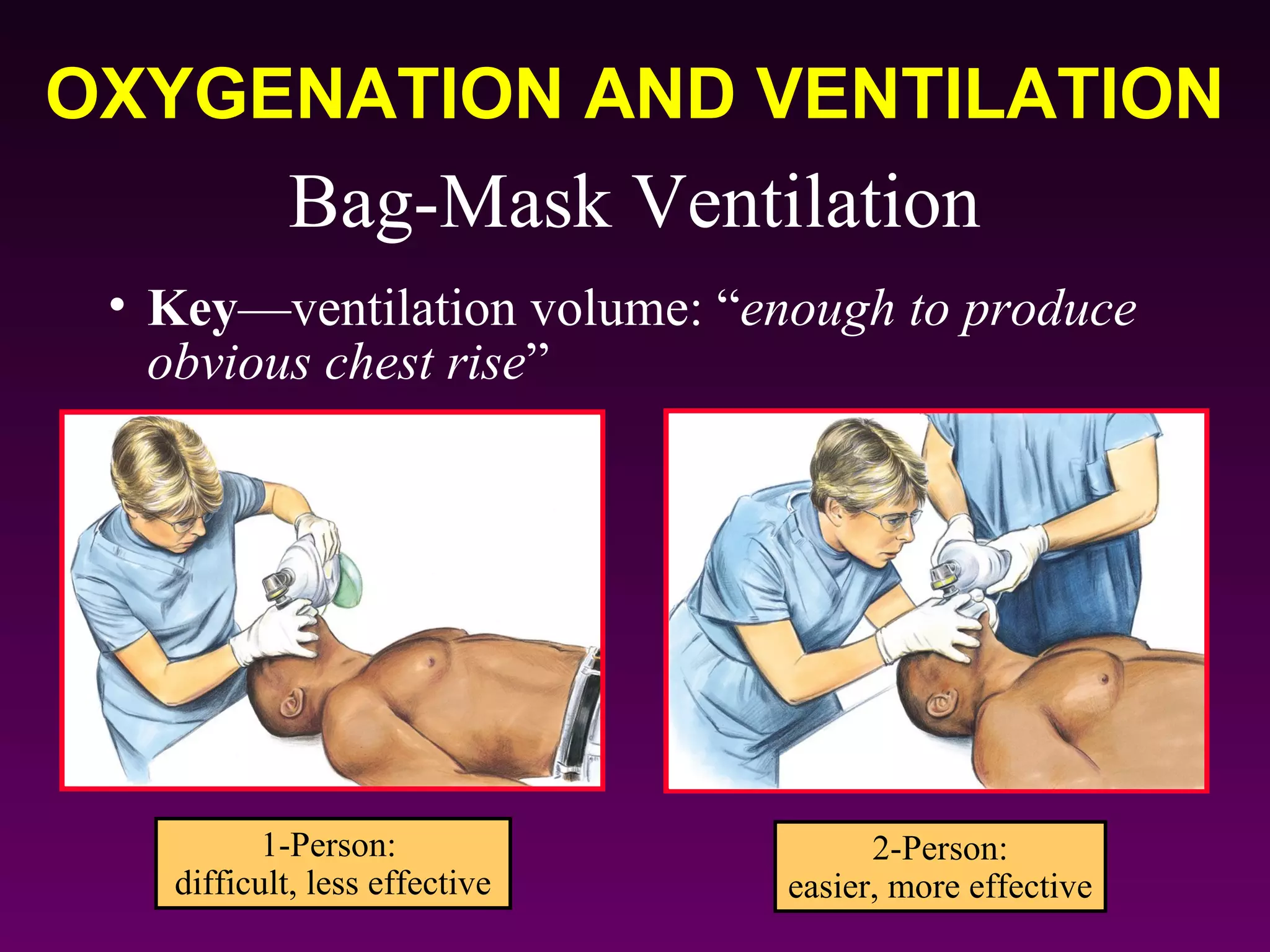
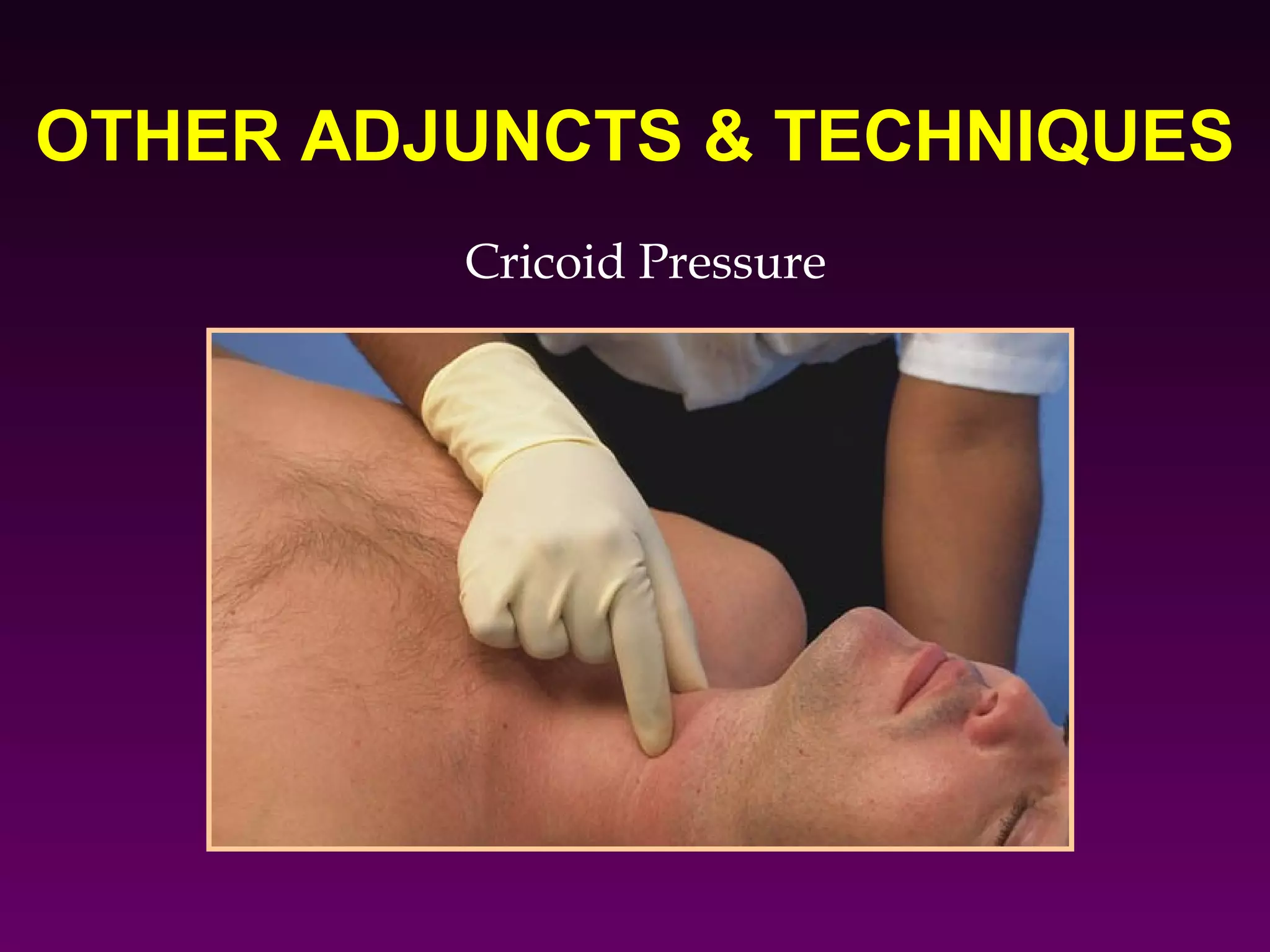
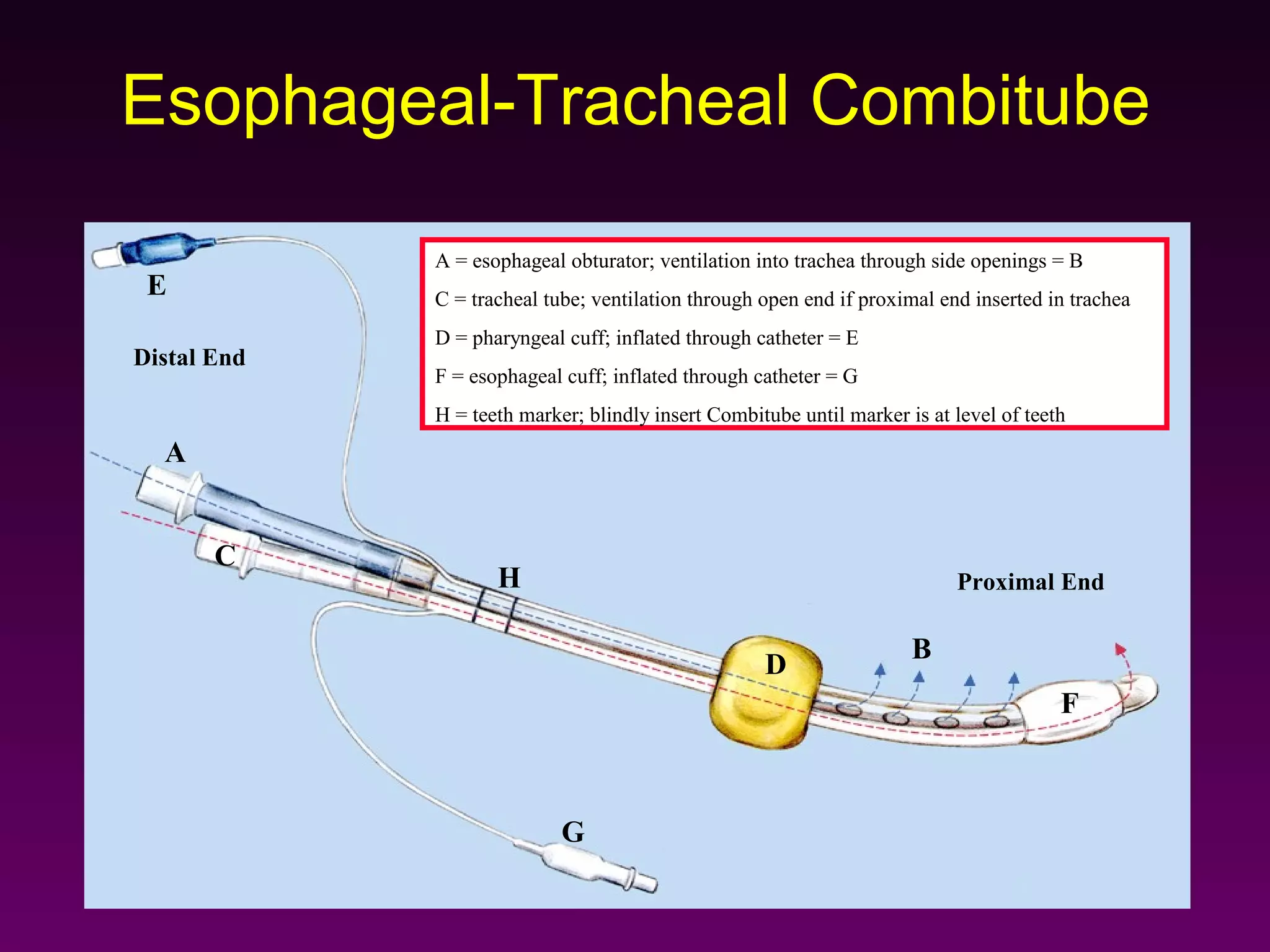
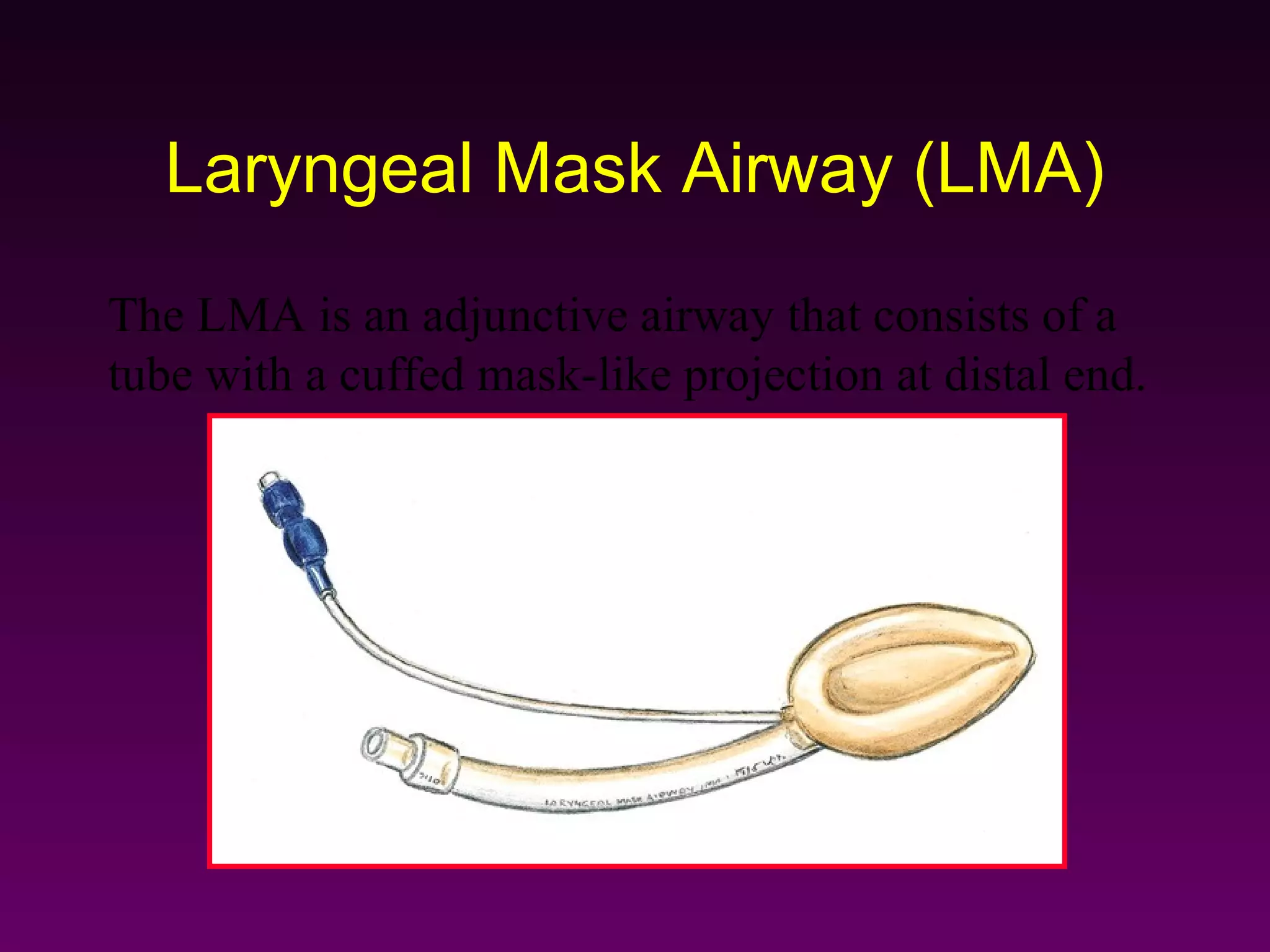
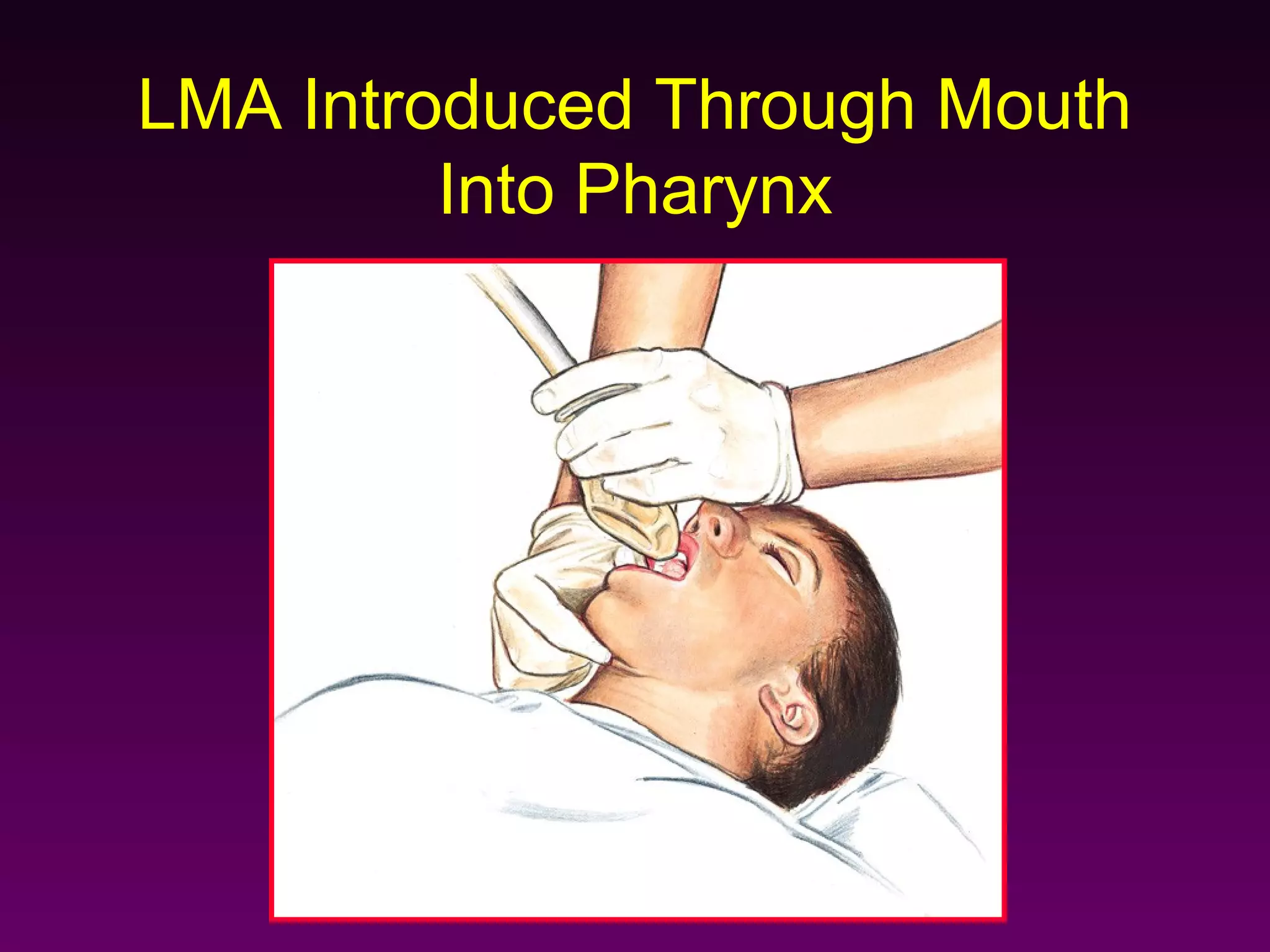
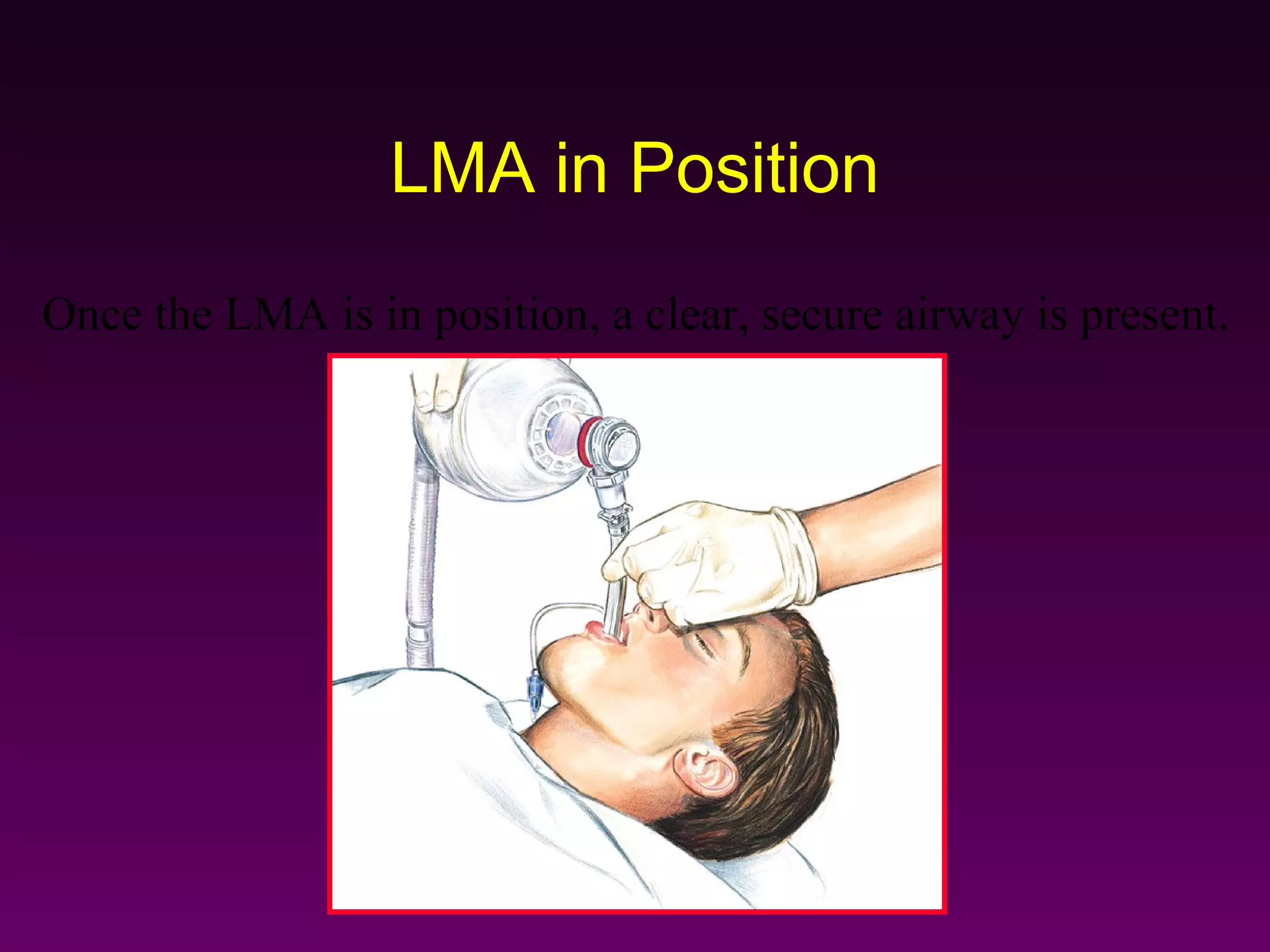
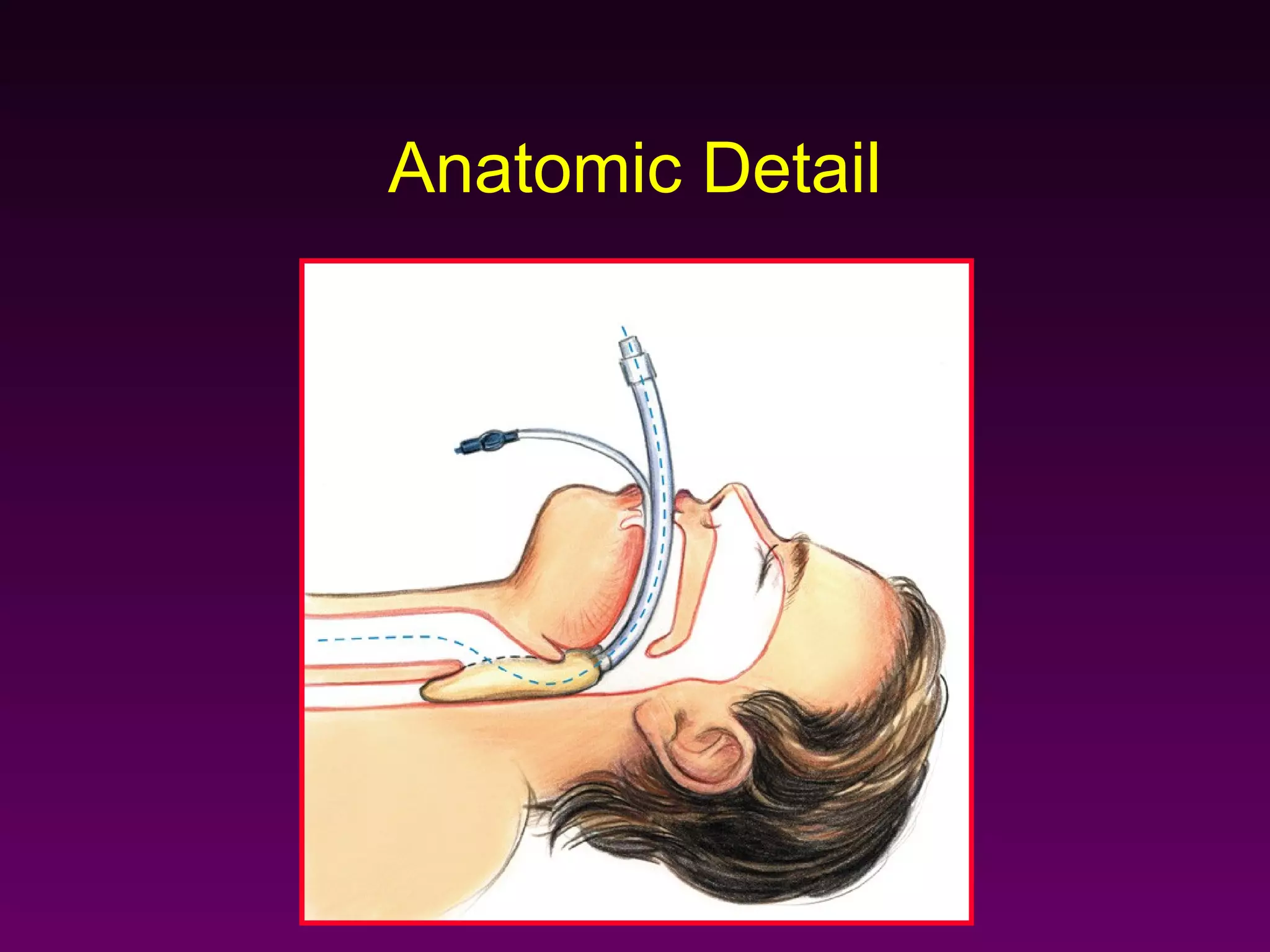
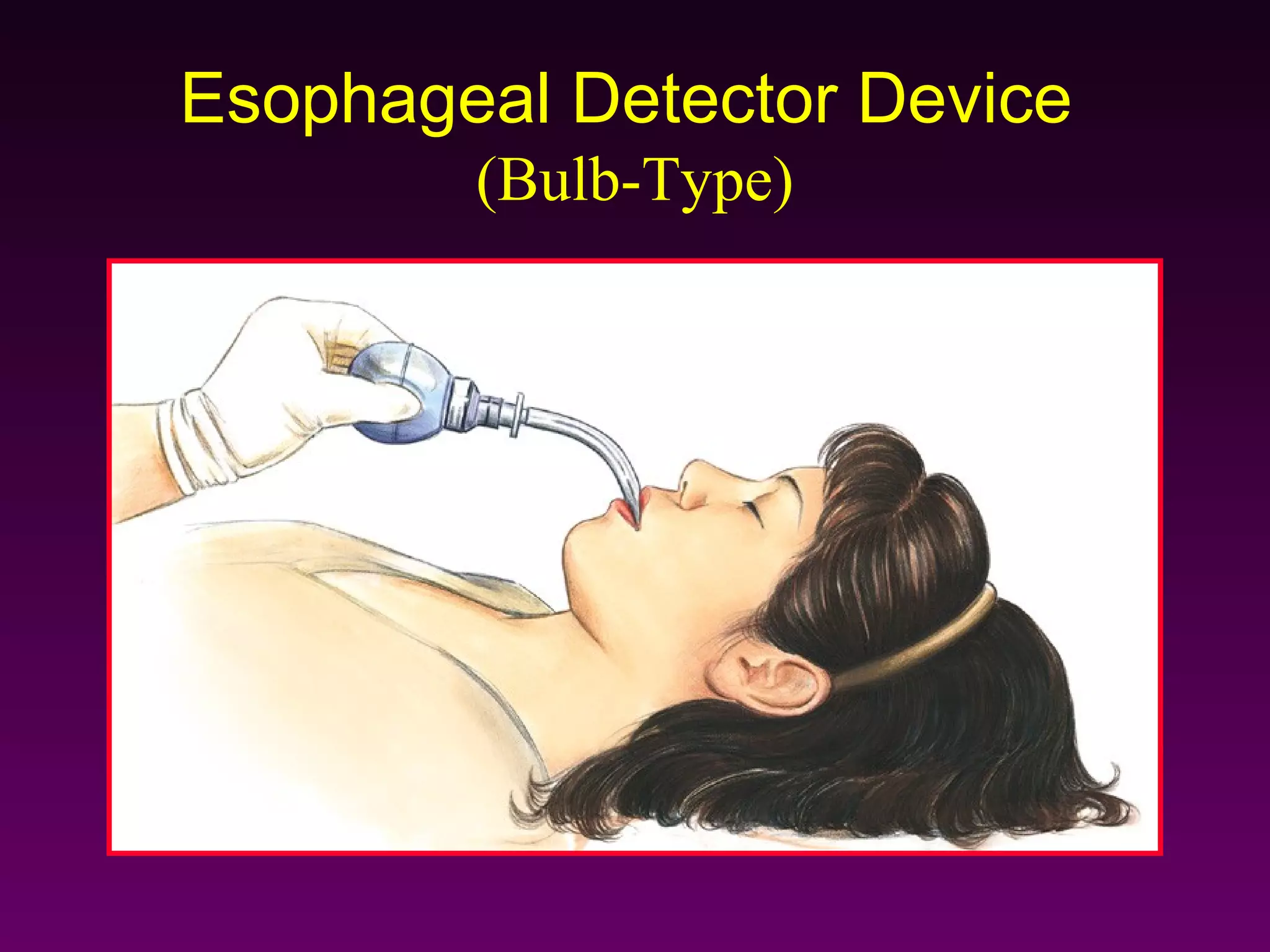
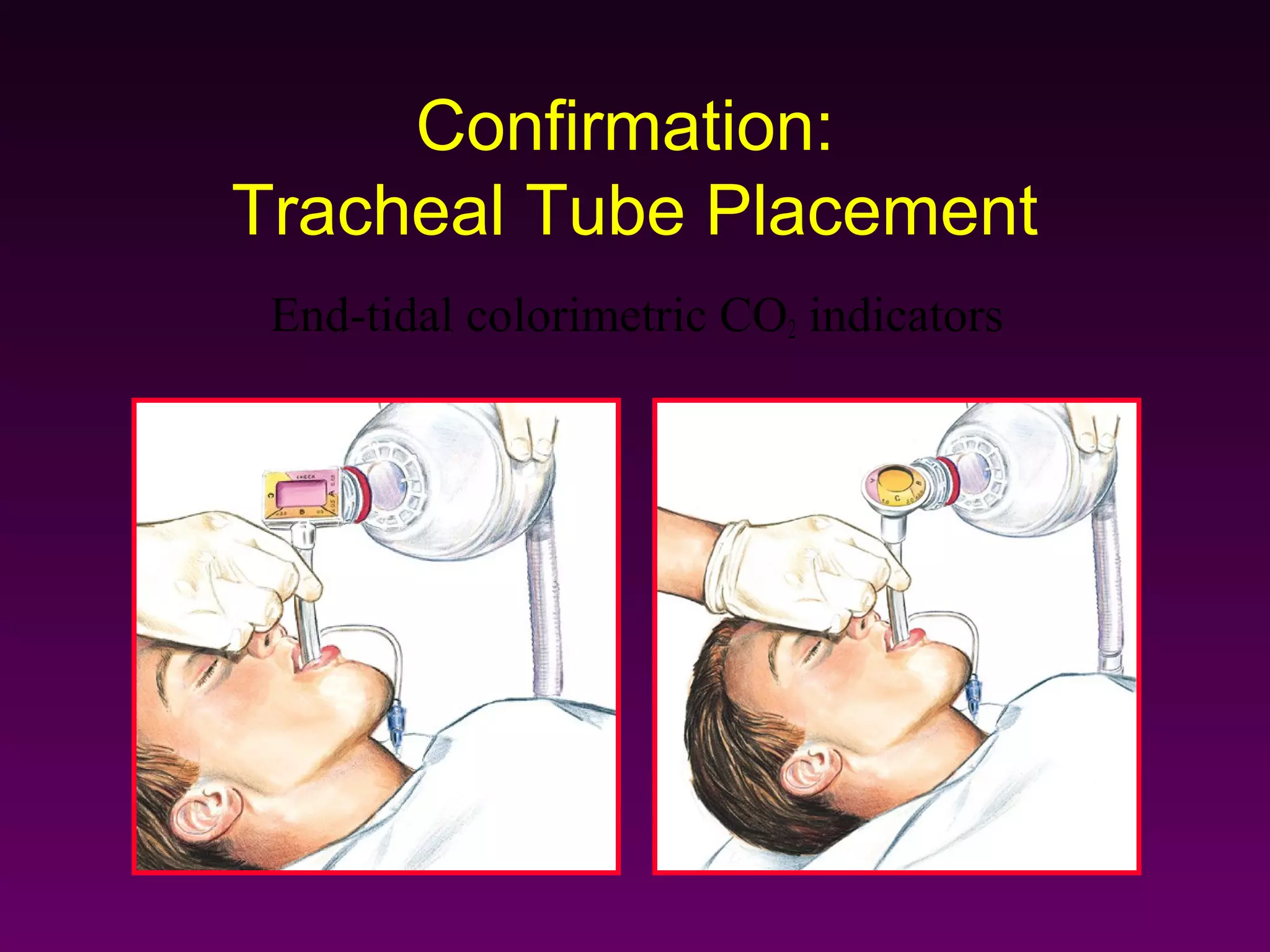
This document provides guidance on using various airway adjuncts, ventilation techniques, and supplemental oxygen during cardiac arrest or respiratory failure. It describes how to open the airway, insert oropharyngeal and nasopharyngeal airways, perform endotracheal intubation, use bag-valve-mask ventilation and mouth-to-mask techniques, provide tracheobronchial suctioning, and confirm proper tracheal tube placement. The goal is to control the airway, optimize ventilation, and effectively deliver supplemental oxygen during emergencies."