Salivary glands and saliva
•Download as PPTX, PDF•
13 likes•2,240 views

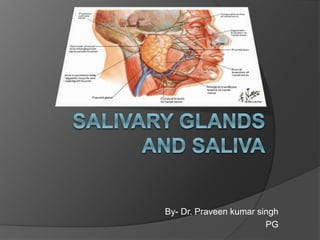
The document provides information about salivary glands and saliva. It discusses the anatomy, histology, physiology and functions of saliva. There are three pairs of major salivary glands - the parotid, submandibular and sublingual glands. Saliva is composed of water, electrolytes, enzymes and other proteins. It is produced for lubrication, digestion and protection of teeth and oral cavity. The parotid gland is the largest salivary gland located below and in front of the ear. The submandibular gland is the second largest, located under the jaw bone. The sublingual gland is the smallest, located under the tongue.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Salivary glands and saliva
Similar to Salivary glands and saliva (20)
Recently uploaded
Recently uploaded (20)
Salivary glands and saliva
- 1. By- Dr. Praveen kumar singh PG
- 2. Contents Introduction Anatomy Development Histology Physiology Functions of saliva Applied Phsiology
- 3. INTRODUCTION The oral cavity is a moist environment, a film of fluid called saliva constantly coats its inner surfaces and occupies the space between the lining oral mucosa and the teeth. Saliva is a complex fluid, produced by the salivary glands, whose important role is maintaining the wellbeing of the mouth. Patients with a deficiency of salivary secretion experience difficulty eating, speaking, swallowing as well as become prone to mucosal infections and rampant caries.
- 4. ANATOMY of salivary glands
- 5. ANATOMY There are three pairs of major salivary glands. 1. Parotid glands 2. Submandibular glands 3. Sublingual glands. There are more than 400 minor salivary glands (labial, lingual, palatal, buccal, glossopalatine and retromolar).
- 6. Parotid gland FEATURES=> Para-around ; otic-ear It is the largest salivary gland It wieghs about 15 gm Situated below the external acoustic meatus, between the ramus of the mandible and sternocliedomastoid. A part of this forward extension deattched and known as accessory parotid and it lies between the zygomatic arch and the parotid duct.
- 7. Capsule of the parotid gland Investing layer of the deep cervical fascia forms capsule for the gland. Fascia splits to enclose the gland. The superficial lamina is thick and adherent to the gland and attached above to the zygomatic arch. The deep lamina is thin and is attached to the styloid process, the angle and the posterior border of the ramus of the mandible and the tympanic plate.
- 8. A portion of deep lamina extending between the styloid process and the mandible is thickened to form the stylomandibular ligamnet which separates the parotid gland from the submandibular salivary gland. The ligament is pierced by the external carotid artery.
- 9. External features The gland resembles three sided pyramid. Apex of pyramid is directed downwards . The gland has four surfaces:- Superior(base of pyramid) Superficial Anteriomedial posteromedial
- 10. The surfaces are separated by three borders: Anterior Posterior Medial/pharyngeal
- 11. Relations -
- 13. Structures within the gland a. Arteries b. Veins
- 14. c. Facial nerve Pattern of branching is called pes anserinus Patey’s faciovenousplane
- 15. d. Parotid lymph nodes
- 16. Parotid duct/ stenson’s duct It is thick walled and about 5 cm long. It emerges from the middle of the anterior border of the gland. It runs forward and slightly downwards on the masseter.
- 17. Stenson’s duct relations are:- Superiorly:- Accesory parotid gland Transverse facial vessels Upper buccal branch of the facial nerve Inferiorly Buccal fat pad Buccopharyngeal fascia Buccinator (obliuquely)
- 18. Blood supply: Arterial: o External carotid artery o Its terminal branches o Posterior auricular o Superficial temporal o Transverse facial arteries Venous: Retromandibular vein
- 19. Lymph drainage: Into parotid lymph nodes and deep cervical lymph nodes.
- 20. Autonomic nerve innervation 1. Parasympathetic secretomotor fibers from the inferior salivatory nucleus of the ninth cranial nerve supply the parotid gland. The nerve fibers pass to the otic ganglion via the tympanic branch of the ninth cranial nerve and the lesser petrosal nerve. 2. Postganglionic parasympathetic fibers reach the parotid gland via the auriculotemporal nerve, which lies in contact with the deep surface of the gland.
- 21. Post-ganglionic sympathetic fibers reach the gland as a plexus of nerves around the external carotid artery.
- 23. Sympathetic nerves are vasomotor and are derived from the plexus around the middle meningeal artery. Sensory nerves to the gland come from the auriculotemporal nerve, but the parotid fascia is innervated by the great auricular nerve (C2, C3).
- 24. Applied aspects Parotid swellings are very painful due to the underlying nature of the parotid fascia. The lobule of the ear is often pushed up in parotid swelling Mumps is infection of salivary gland caused by paromyxovirus which will cause severe pain
- 25. A parotid abscess may be caused by the spread of infection from the oral cavity. An infection may also spread due to the parotid lymph node draining an infected area. For tumours of the parotid gland incision biopsy is not indicated as it will cause the seeding of the tumour .
- 26. Parotidectomy is the removal of the parotid gland. After this operation at times there may be regeneration of the secretomotor fibres in the auriculotemporal nerve which join the great auricular nerve. This causes stimulation of the sweat glands and hyperaemia in the area of its distribution thus producing redness and sweating in the area of skin supplied by the nerve.
- 27. This clinical entity is called FREY SYNDROME. Whenever such a person chew there is increase in the sweating in the region supplied by auriculotemporal nerve. So it is called auriculotemporal syndrome
- 28. Submandibular salivary gland Second largest salivary gland Situated in the anterior part of the the diagastric traingle Gland is size of walnut It is roughly J-shaped
- 29. Superficial part Inferior surfaces Lateral surface Medial surfaces The gland is enclosed to between two layers of deep cervical fascia.
- 30. Relations Inferior surface is covered by:- Skin Platysma Cervical branch of the facial nerve Deep fascia Facial vein Submandibular lymph nodes
- 31. Lateral surface related to:- Submandibular fossa related to the mandible Insertion of the medial pterygoid Facial artery
- 32. Medial surface related to the:- Mylohyoid Hyoglossus Styloglossus muscle Inferiorly : it overlaps stylohyoid and the posterior belly of the diagastric.
- 33. Deeper part Small in size Situated deep to the mylohyoid line and superficial to the hyoglossus and styloglossus Posteriorly, it is continuous with the superficial part round the posterior border of the mylohyoid. Anteriorly, it extends up to the posterior end of the sublingual gland
- 34. Relations Present in between mylohyoid and hyoglossus Laterally- Mylohyoid Medially- Hyoglossus Above – lingual nerve with sub mandibular ganglion Below – Hypoglossal nerve
- 35. Relation to facial vein and artery---
- 36. Submandibular duct / wharton’s duct Thin walled and is about 5 cm long. Emerges from the anterior end of the deeper part of the gland. Runs forward to the hyoglossus between the lingual and hypoglossal nerves. At the anterior border of the hyoglossus, duct is crossed by the lingual nerve. Opens in the floor of the mouth on the summit of sublingual papilla, at the side of the frenulum of the tongue.
- 37. Opening of wharton’s duct
- 38. BLOOD SUPPLY(ARTERIAL) Submental and sublingual arteries. Facial artery. Lingual artery. BLOOD SUPPLY(VENOUS) Anterior facial vein. Common facial vein. LYMPHATIC DRAINAGE Submandibular lymph nodes.
- 39. NERVE SUPPLY
- 40. Vasomotor sympathetis- fibres from the plexus on the facial artery. Sensory fibres - Lingual nerve.
- 41. Applied aspects The formation of calculus is more common in the submandibular gland than in the parotid. A stone in the submandibular duct(wharton’s duct) can be palpated bimanually in the floor of the mouth and can even be seen if sufficiently large.
- 42. Sublingual salivary gland Smallest of the three salivary gland Almond shaped and weighs about 3 to 4 gm
- 43. Lies above the mylohyoid below the mucosa of the floor of the mouth, medial to sublingual fossa of the mandible and lateral to the genioglossus.
- 44. Relations Front- meet with the opposite side gland Behind – comes in contact with the deeper part of the submandibular gland Above- mucous membrane of the mouth Below- mylohyoid muscle Lateral- sublingual fossa Medial- genioglossus muscle
- 45. Sublingual gland has no true fascial capsule. It lacks a single dominant duct. Instead, it is drained by approximately 10 - 12 small ducts (the Ducts of Rivinus). Ducts of Rivinius either secrete directly into floor of mouth or empty into BARTHOLIN’s duct that then continues into Wharton’s duct. The gland receives blood supply from the lingual and submental arteries. Nerve supply is similar to that of submandibular gland
- 46. Applied aspects The structures at risk during dissection of the gland are the submandibular duct and the lingual nerve. The duct lies superficially in the floor of the mouth medial to the sublingual fold, and is crossed inferiorly by the nerve which then enters the tongue The sublingual artery and vein also lie on the medial aspect of the gland close to the submandibular duct and lingual nerve.
- 47. Minor salivary glands About 600 to 1,000 minor salivary glands, ranging in size from 1 to 5 mm, line the oral cavity and oropharynx. These lie just under mucosa. Distributed over lips, cheeks, palate, floor of mouth & retro-molar area. Also appear in upper aero-digestive tract Contribute 10% of total salivary volume.
- 48. DEVELOPMENT of salivary glands
- 49. The salivary glands develop as outgrowth of the buccal epithelium. The outgrowths are at first solid and are later canalised. They branch repeatedly to form the duct system. The terminal parts of the duct system develop into secretory acini.
- 50. As the salivary glands develop near the junctional area between the ectoderm of the foregut, it is difficult to determine whether they are ectodermal or endodermal. The outgrowth for the parotid gland arises in relation to the line along which the maxillary and mandibular process fuse to form the cheek. it is generally cosidered as ectodermal.
- 51. The outgrowths for the submandibular and sublingual glands arise in relation to the linguo- gingival sulcus. They are usually cosidered to be of endodermal origin.
- 53. Histology of salivary glands
- 54. Structure of salivary glands The working parts of the salivary glandular tissue consist of the secretory end pieces (acini) and the branched ductal system. In serous glands (e.g. the parotids) the cells in the end piece are arranged in a roughly spherical form. In mucous glands, they tend to be arranged in a tubular configuration with a larger central lumen.
- 55. In both types of gland the cells in the end piece surround a lumen and this is the start of the ductal system. There are three types of duct present in all salivary glands. Intercalated duct Striated duct Excretory duct
- 56. The fluid first passes through the intercalated ducts which have low cuboidal epithelium and a narrow lumen. From there the secretions enter the striated ducts which are lined by more columnar cells with many mitochondria. Finally, the saliva passes through the excretory ducts where the cell type is cuboidal until the terminal part which is lined with stratified squamous epithelium.
- 57. End pieces may contain mucous cells, serous cells or a mixture of both. A salivary gland can consist of a varied mixture of these types of end pieces. In mixed glands, the mucous acini are capped by a serous demilune. In addition, myoepithelial cells surround the end piece, their function being to assist in propelling the secretion into the ductal system. The gland and its specialised nerve and blood supply are supported by a connective tissue stroma.
- 58. Differences:- Serous acini Mucous acini 1. Samller in size,rounded in shape. 2. Lumen hardly visible. 3. Lining cells pyramidal in shape and relatively more in number. 4. Nuclie are round and basal. 5. Cytoplasm depicts basal basophilia and apical eosinophilia. 6. May present as demilunes on one aspect of some mucous acini 1. Larger in size , more variable in shape. 2. Lumen mostly visible. 3. Lining cells truncated columnar in shape. Cells relatively fewer in number. 4. Nuclie are flattened and peripheral. 5. Cytoplasm is pale and vacuolated. 6. Mucous acini only present as complete acini.
- 63. Physiology of saliva Composition- Saliva is slightly cloud in appearance due to the presence of cells and mucin. Saliva is slightly acidic and the Ph varies from 6.7 to 7.4, specific gravity is 1.002 to 1.012. The resting rate of saliva is on an average is about 0.3 to 0.4 ml/min.. Saliva contains about 99.5% of water and 0.5% of solid.
- 64. Solid present in saliva consists:- Cellular costituents – consist of yeast, bacteria, protozoa, polymorphonuclear leukocytes and desquamated epithelial cells. Inorganic ions- major(Na + ,k+ ,Cl-,HCO3-) and Minor (Ca++ ,Mg++ ,HPO4-, I, Scn- and F-)
- 65. Secretory proteins and glycoprotiens – various enzymes, large carbohydrte rich protien or mucin, antibacterial substance, group of protiens involved in enamel. Serum constituents- albumin, blood clotting factor , B2 microglobulin and immunoglobulin.
- 67. Source of saliva- Saliva is secreted from the salivary glands: via parotid gland-25%; submandibular gland – 70% ; sublingual gland – 5% Minor salivary gland present on palate , buccal mucosa, and tongue also produce modest amounts of saliva.
- 68. Normal stimulated flow of saliva- for different ages can be calculated by the equation:- 0.78 * age + 5.6 = stimulated flow / 15 min 5.6 – it is stimulated flow of the infants
- 69. Secretion of saliva Although fluid secretion occurs only through the acini, proteins are produced and transported into the saliva through both acinar and ductal cells. The primary saliva within the acinar end pieces is isotonic with serum but undergoes extensive resorption of sodium and chloride and secretion of potassium within the duct system. The saliva, as it enters the oral cavity, is a protein-rich hypotonic fluid.
- 70. The secretion of saliva is controlled by sympathetic and parasympathetic neural input. The stimulus for fluid secretion is primarily via muscarinic-cholinergic receptors, whereas the stimulus for protein release occurs largely through b-adrenergic receptors. Salivary cells also display an array of additional receptors that influence secretory functions.
- 71. Activation of these receptors induces a complex signaling and signal transduction pathway within the cells, involving numerous transport systems, resulting in a tightly regulated secretion process. Mobilization and regulation of intracellular calcium are a critical component of this process within the secretory cells.
- 72. Nervous Regulation of Salivary Secretion The salivary glands are controlled mainly by the parasympathetic nervous signals all the way from the superior and inferior salivatory nuclei in the brain stem. The salivatory nucleus located at the juncture of the medulla and pons and are excited by both taste and tactile stimuli from the tongue and other areas of the mouth and pharynx.
- 73. Sour taste stimuli elict the saliva secretion 8 to 20 times than the basal rate. Salivation can also be stimulated or inhibited by nervous signals arriving in the salivatory nuclei from higher centres of the central nervous system. The appetite area of the brain , which partially regulates secretion is located in proximity to the parasympathetic centres of the hypothalmus, and it function to great extent in response to signals from the taste and smell area of cerebral cortex or amygdala.
- 74. Sympathetic stimulation can also increase the salivation a slight amount, much less so than does parasympathetic stimulation. The sympathetic nerves originate from the superior cervical ganglia and travel along the surfaces of the blood vessels walls of the salivary glands.
- 76. Functions of saliva Function Action Fluid/Lubricant Coats hard and soft tissue which helps to protect against mechanical, thermal and chemical irritation and tooth wear. Assists smooth air flow, speech and swallowing. Ion reservoir Solution supersaturated with respect to tooth mineral facilitates remineralisation of the teeth. Statherin and acidic proline-rich proteins in saliva inhibit spontaneous precipitation of calcium phosphate salts. Buffer Helps to neutralise plaque pH after eating, thus reducing time for demineralisation. Cleansing Clears food and aids swallowing. Antimicrobial actions Specific (e.g. sIgA) and non-specific (e.g. Lysozyme,Lactoferrin and Myeloperoxidase) anti-microbial mechanisms help to control the oral microflora. Agglutination Agglutinins in saliva aggregate bacteria, resulting in accelerated clearance of bacterial cells. Examples are mucins and parotid saliva glycoproteins.
- 77. Pellicle formation Thin (0.5 μm) protective diffusion barrier formed on enamel from salivary and other proteins. Digestion The enzyme α-amylase is the most abundant salivary enzyme; it splits starchy foods into maltose, malto-triose and dextrins. Taste Saliva acts as a solvent, thus allowing interaction of foodstuff with taste buds to facilitate taste Excretion As the oral cavity is technically outside the body, substances which are secreted in saliva are excreted. This is a very inefficient excretory pathway as reabsorption may occur further down the intestinal tract. Water balance Under conditions of dehydration, salivary flow is reduced, dryness of the mouth and information from osmo-receptors are translated into decreased urine production and increased drinking.
- 78. „APPLIED PHYSIOLOGY HYPOSALIVATION Reduction in the secretion of saliva is called hyposalivation. It is of two types, namely temporary hyposalivation and permanent hyposalivation. 1. Temporary hyposalivation occurs in: i. Emotional conditions like fear. ii. Fever. iii. Dehydration.
- 79. 2. Permanent hyposalivation occurs in: i. Sialolithiasis (obstruction of salivary duct). ii.Congenital absence or hypoplasia of salivary glands. iii. Bell palsy (paralysis of facial nerve).
- 80. HYPERSALIVATION Excess secretion of saliva is known as hypersalivation. Physiological condition when hypersalivation occurs is pregnancy. Hypersalivation in pathological conditions is called ptyalism, sialorrhea, sialism or sialosis.
- 81. Hypersalivation occurs in the following pathological conditions: 1. Decay of tooth or neoplasm (abnormal new growth or tumor) in mouth or tongue due to continuous irritation of nerve endings in the mouth. 2. Disease of esophagus, stomach and intestine.
- 82. 3.Neurological disorders such as cerebral palsy, mental retardation, cerebral stroke and parkinsonism. 4.Some psychological and psychiatric conditions. 5.Nausea and vomiting.
- 83. OTHER DISORDERS 1. Xerostomia 2. Drooling 3. Chorda tympani syndrome 4. Paralytic secretion of saliva 5. Augmented secretion of saliva 6. Mumps 7. Sjögren syndrome.
- 84. 1. Xerostomia Xerostomia means dry mouth. It is also called pasties or cottonmouth. It is due to hyposalivation or absence of salivary secretion (aptyalism). Causes- i. Dehydration or renal failure. ii. Sjögren syndrome. iii. Radiotherapy. iv. Trauma to salivary gland or their ducts.
- 85. v. Side effect of some drugs like antihistamines, antidepressants, monoamine oxidase inhibitors, antiparkinsonian drugs and antimuscarinic drugs. vi. Shock. vii. After smoking marijuana (psychoactive compound from the plant Cannabis). Xerostomia causes difficulties in mastication, swallowing and speech. It also causes halitosis (bad breath; exhalation of unpleasant odors).
- 86. 2. Drooling Uncontrolled flow of saliva outside the mouth is called drooling. It is often called ptyalism. Causes- Drooling occurs because of excess production of saliva, in association with inability to retain saliva within the mouth.
- 87. Drooling occurs in the following conditions: i. During teeth eruption in children. ii. Upper respiratory tract infection or nasal allergies in children. iii. Difficulty in swallowing. iv. Tonsillitis. v. Peritonsillar abscess.
- 88. 3. Chorda Tympani Syndrome Chorda tympani syndrome is the condition characterized by sweating while eating. During trauma or surgical procedure, some of the parasympathetic nerve fibers to salivary glands may be severed. During the regeneration, some of these nerve fibers, which run along with chorda tympani branch of facial nerve may deviate and join with the nerve fibers supplying sweat glands. When the food is placed in the mouth, salivary secretion is associated with sweat secretion.
- 89. 4. Paralytic Secretion of Saliva When the parasympathetic nerve to salivary gland is cut in experimental animals, salivary secretion increases for first three weeks and later diminishes; finally it stops at about sixth week. The increased secretion of saliva after cutting the parasympathetic nerve fibers is called paralytic secretion. It is because of hyperactivity of sympathetic nerve fibers to salivary glands after cutting the parasympathetic fibers.
- 90. These hyperactive sympathetic fibers release large amount of catecholamines, which induce paralytic secretion. Moreover, the acinar cells of the salivary glands become hypersensitive to catecholamines after denervation. The paralytic secretion does not occur after the sympathetic nerve fibers to salivary glands are cut.
- 91. 5. Augmented Secretion of Saliva If the nerves supplying salivary glands are stimulated twice, the amount of saliva secreted by the second stimulus is more than the amount secreted by the first stimulus. It is because, the first stimulus increases excitability of acinar cells, so that when the second stimulus is applied, the salivary secretion is augmented.
- 92. 6. Mumps Mumps is the acute viral infection affecting the parotid glands. The virus causing this disease is Paramyxovirus. It is common in children who are not immunized. It occurs in adults also. Features of mumps are puffiness of cheeks (due to swelling of parotid glands), fever, sore throat and weakness. Mumps affects meninges, gonads and pancreas also.
- 93. 7. Sjögren Syndrome Sjögren syndrome is an autoimmune disorder in which the immune cells destroy exocrine glands such as lacrimal glands and salivary glands. It is named after Henrik Sjögren who discovered it. Common symptoms of this syndrome are dryness of the mouth due to lack of saliva (xerostomia), persistent cough and dryness of eyes.
- 94. In some cases, it causes dryness of skin, nose and vagina. In severe conditions, the organs like kidneys, lungs, liver, pancreas, thyroid, blood vessels and brain are affected.
- 95. References Human Anatomy volume 3 – B D Chaurasia’s Text book of Oral Medicine – Anil Govindrao Ghom Essential of Medical Physiology sixth edition – K Sembulingam , Prema Sembulingam Text book of Medical Physiology eleventh edition- Guyton & Hall Text book of Histology third edition – Krishna Garg, Indira Bahl, Mohini Kaul Introduction: the anatomy and physiology of salivary glands - Helen Whelton