Downloaded 200 times
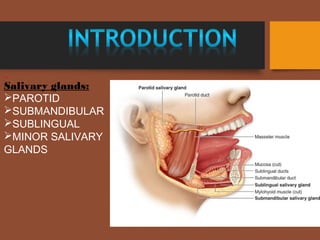
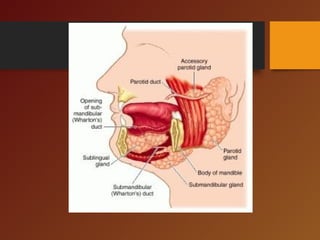

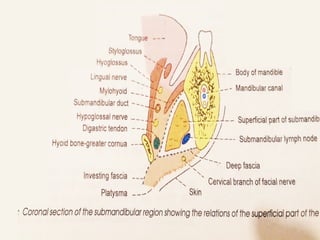
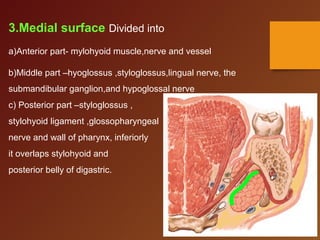
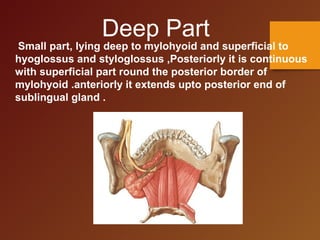
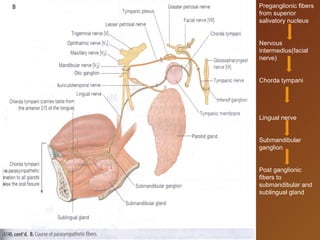


The document discusses the anatomy and clinical considerations of the submandibular gland. It begins by describing the location, structure and relations of the submandibular gland. It then discusses the blood supply, nerve supply, lymphatic drainage and clinical relevance when performing procedures in the submandibular region. The summary concludes by mentioning sialolithiasis, which are salivary stones that can form in the submandibular gland and cause obstruction.



































































