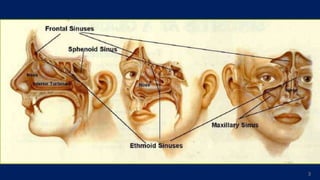
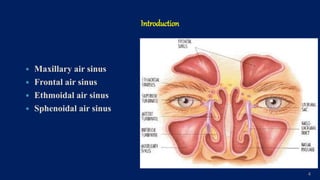
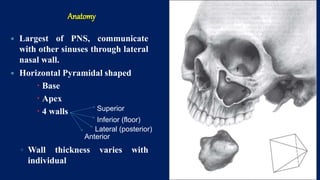
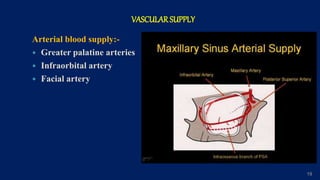
The maxillary sinus is the largest of the paranasal sinuses. It is located within the body of the maxilla bone and communicates with the nasal cavity via an opening called the osteum. The maxillary sinus develops during fetal development and reaches its maximum size around 18 years of age. It has thin walls that are in close proximity to important structures like the orbit and teeth. Conditions like sinusitis or cysts can develop within the maxillary sinus and spread to surrounding areas due to its anatomical relationships. Precise knowledge of the maxillary sinus anatomy is important for dental surgeons to avoid complications during procedures involving nearby teeth.



















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








