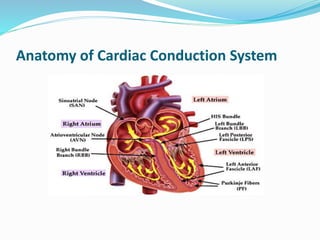
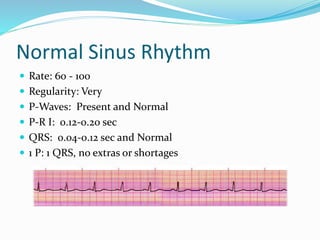
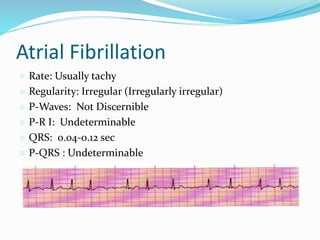
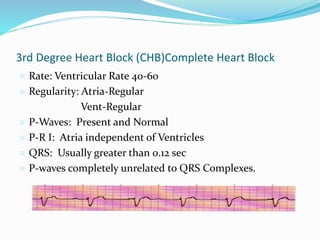
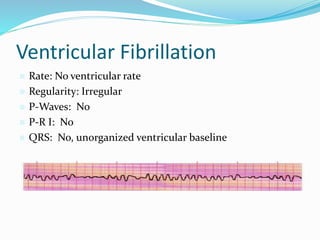
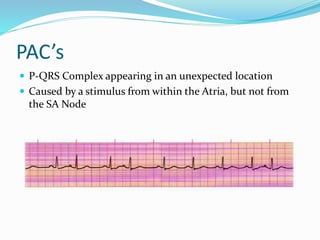
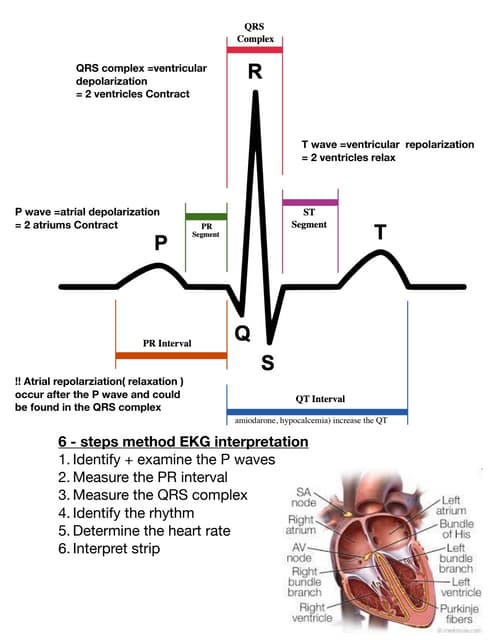
This document provides an overview of cardiac conduction systems, electrocardiograms, arrhythmias, and how to interpret ECG readings. It defines common arrhythmias like sinus tachycardia, atrial fibrillation, ventricular tachycardia and discusses how to identify them using a 6-step approach examining rate, rhythm, P-waves, P-R interval, QRS complex and the relationship between P-waves and QRS. Examples are given of normal sinus rhythm and various arrhythmias with their characteristic ECG patterns. Special situations and normal variants are also addressed.