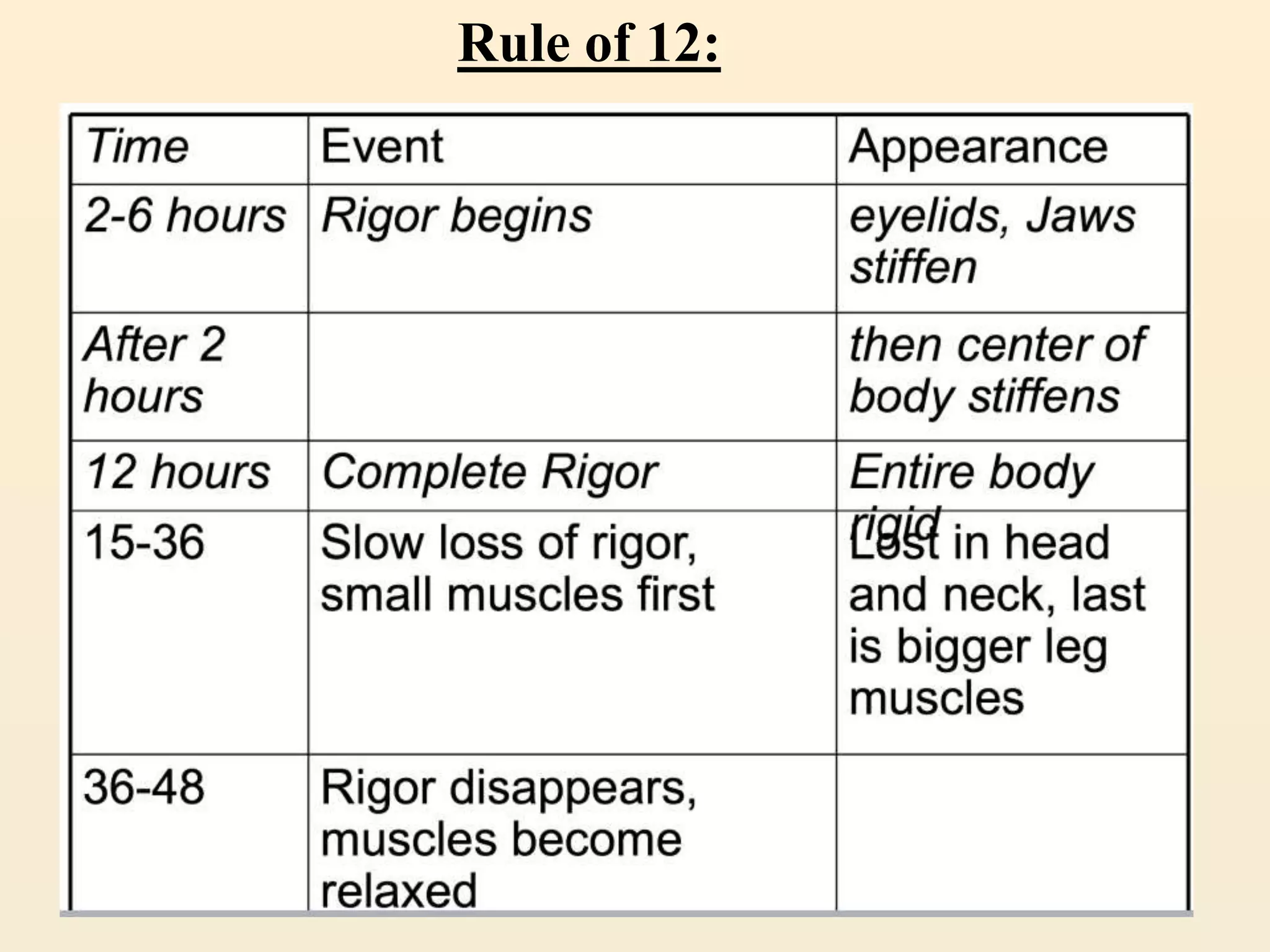
Rigor mortis is the stiffening of muscles that occurs after death. It begins between 2-6 hours after death as ATP is no longer replenished and calcium causes perpetual muscle contraction. Rigor mortis reaches a maximum at around 12 hours and dissipates around 24-72 hours post-mortem. Several factors can alter its onset and duration including temperature, muscle exertion prior to death, and diseases. It is one sign used to estimate time of death but varies considerably between individuals.