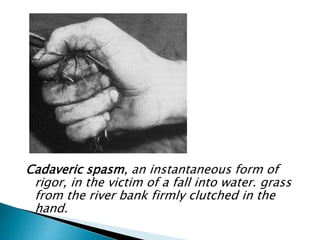
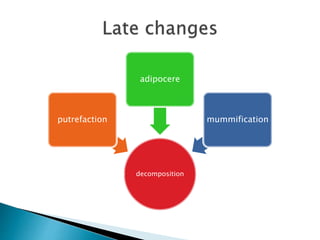
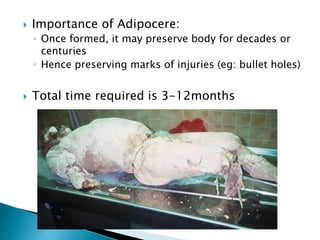
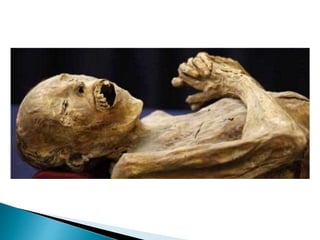
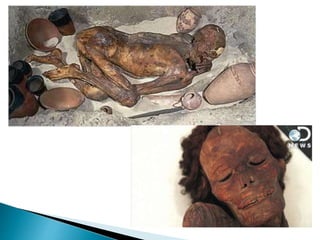
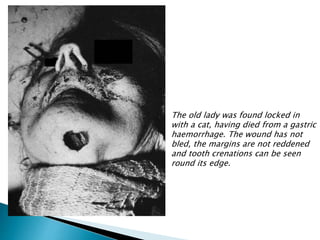
This document discusses various stages of death and decomposition of the human body. It describes somatic or clinical death, which is the irreversible loss of brain and bodily functions. Following ischemia and anoxia, tissues begin to die from cardiorespiratory failure within 1-2 hours. Cells and tissues apart from damaged areas remain alive. Cortical death involves loss of higher brain functions while brainstem death involves loss of vital centers controlling respiration. Decomposition begins with rigor mortis within 6-12 hours as ATP levels fall, followed by hypostasis or livor mortis as blood settles in the lowest parts of the body. Later stages include putrefaction driven by bacterial growth, adipocere formation in moist environments, and












![ Most popular used: Glaister equation
2+ [98.4 F – measured rectal temperature (F)] = Hour
1.5
or
In celcius
2 + [(36.9c – measured rectal temperature ) x 1.2]](https://image.slidesharecdn.com/pmchanges-drfadhil-170108071513/85/Post-mortem-changes-59-320.jpg)