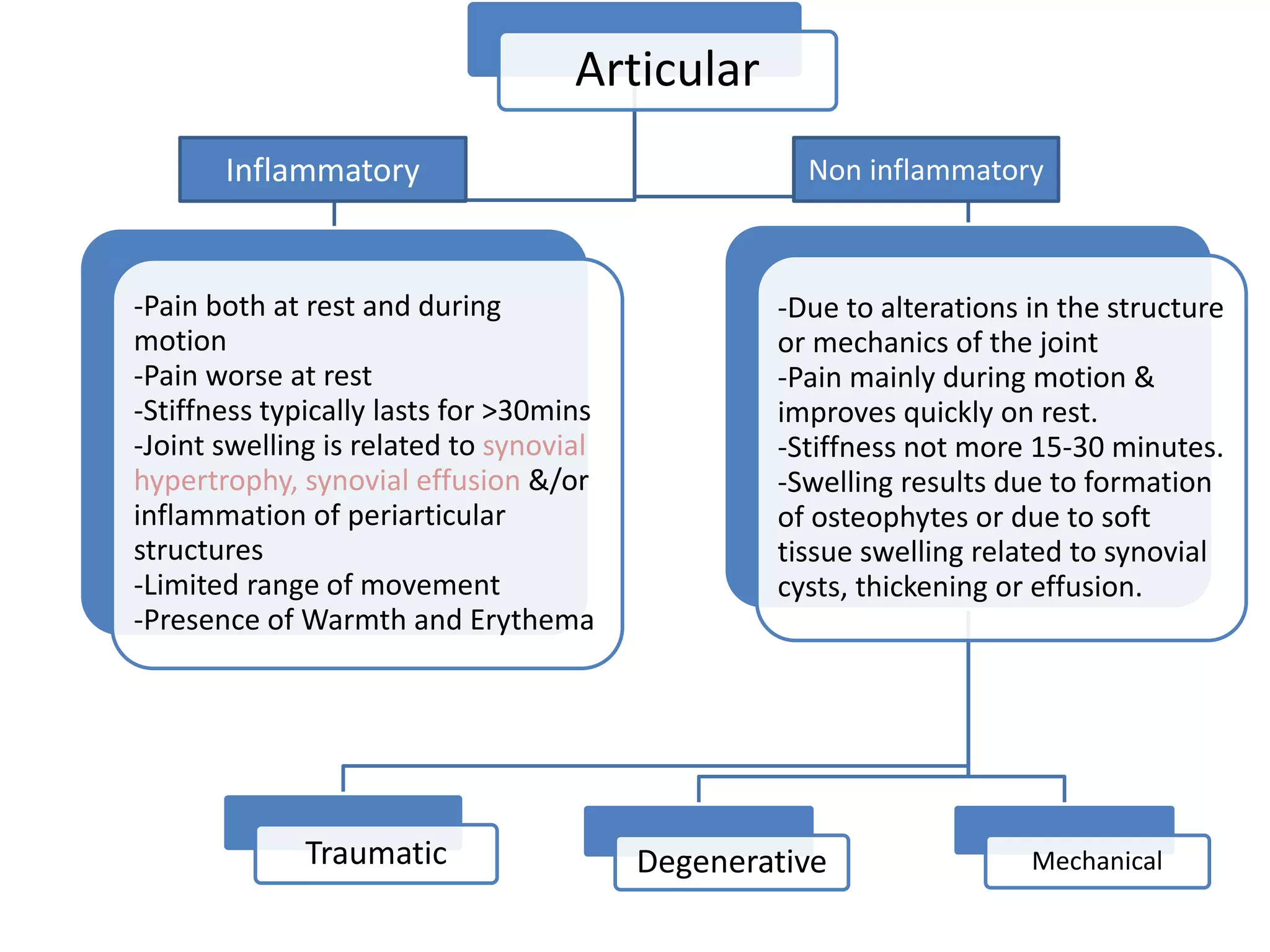
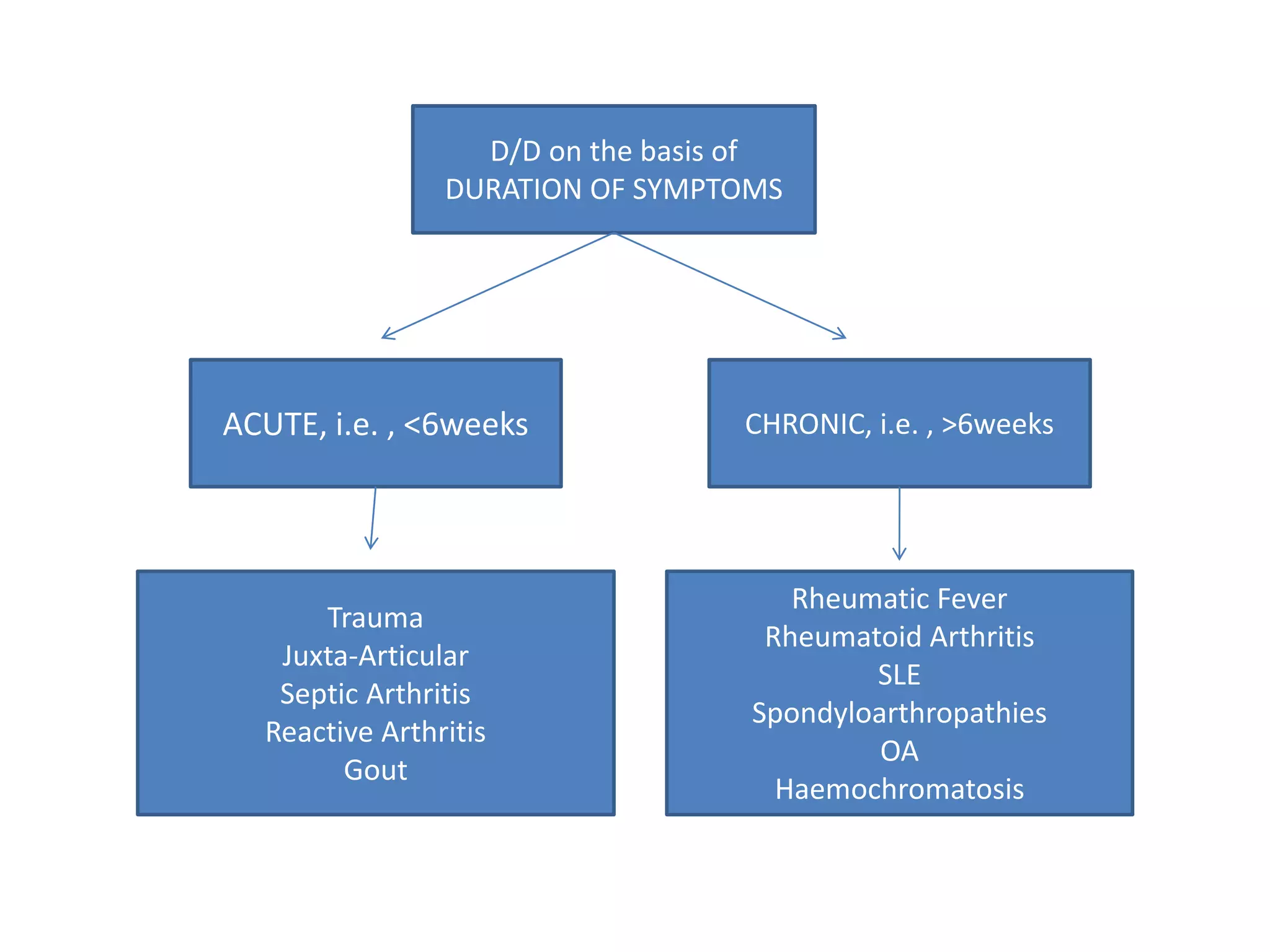
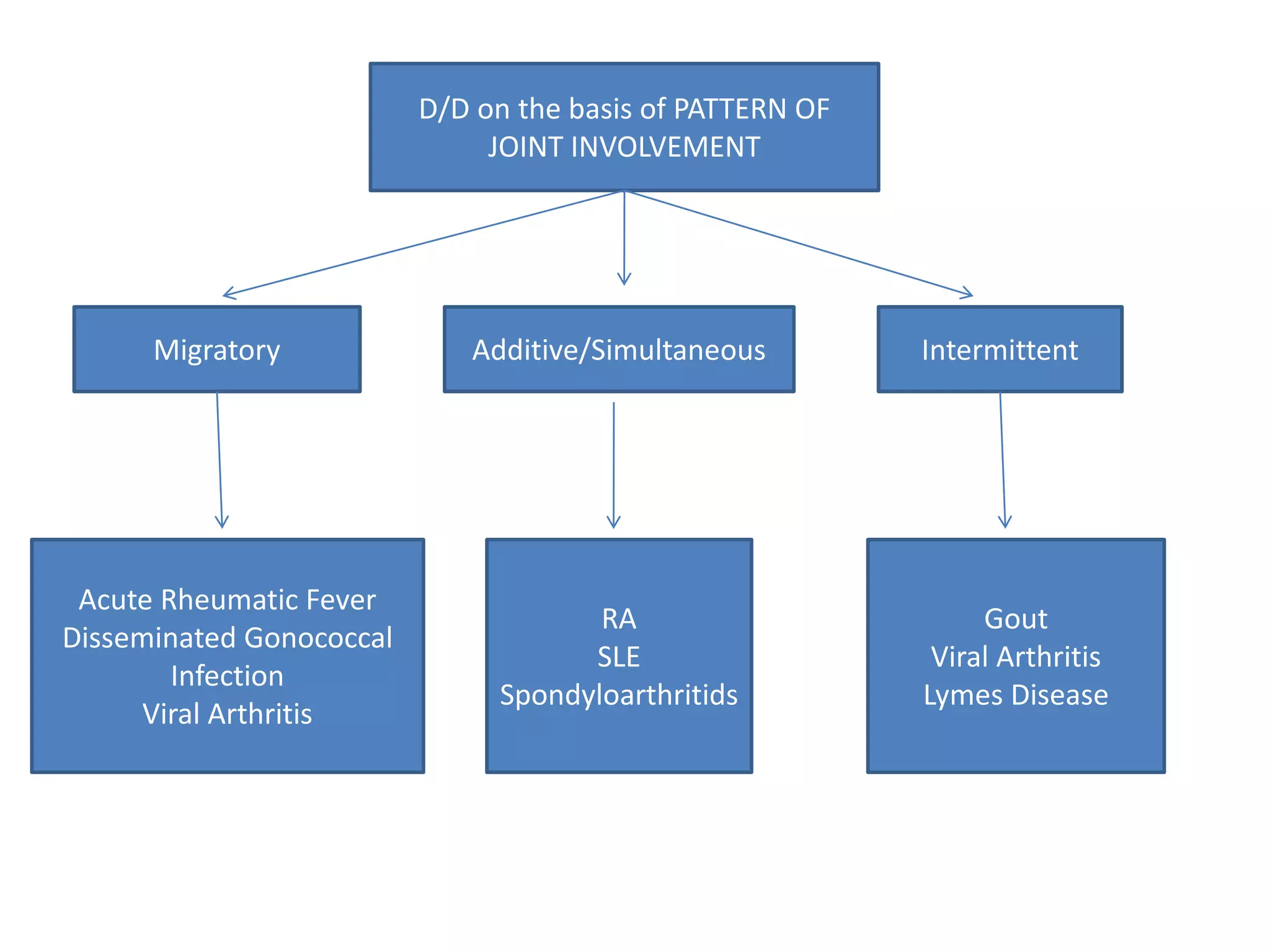
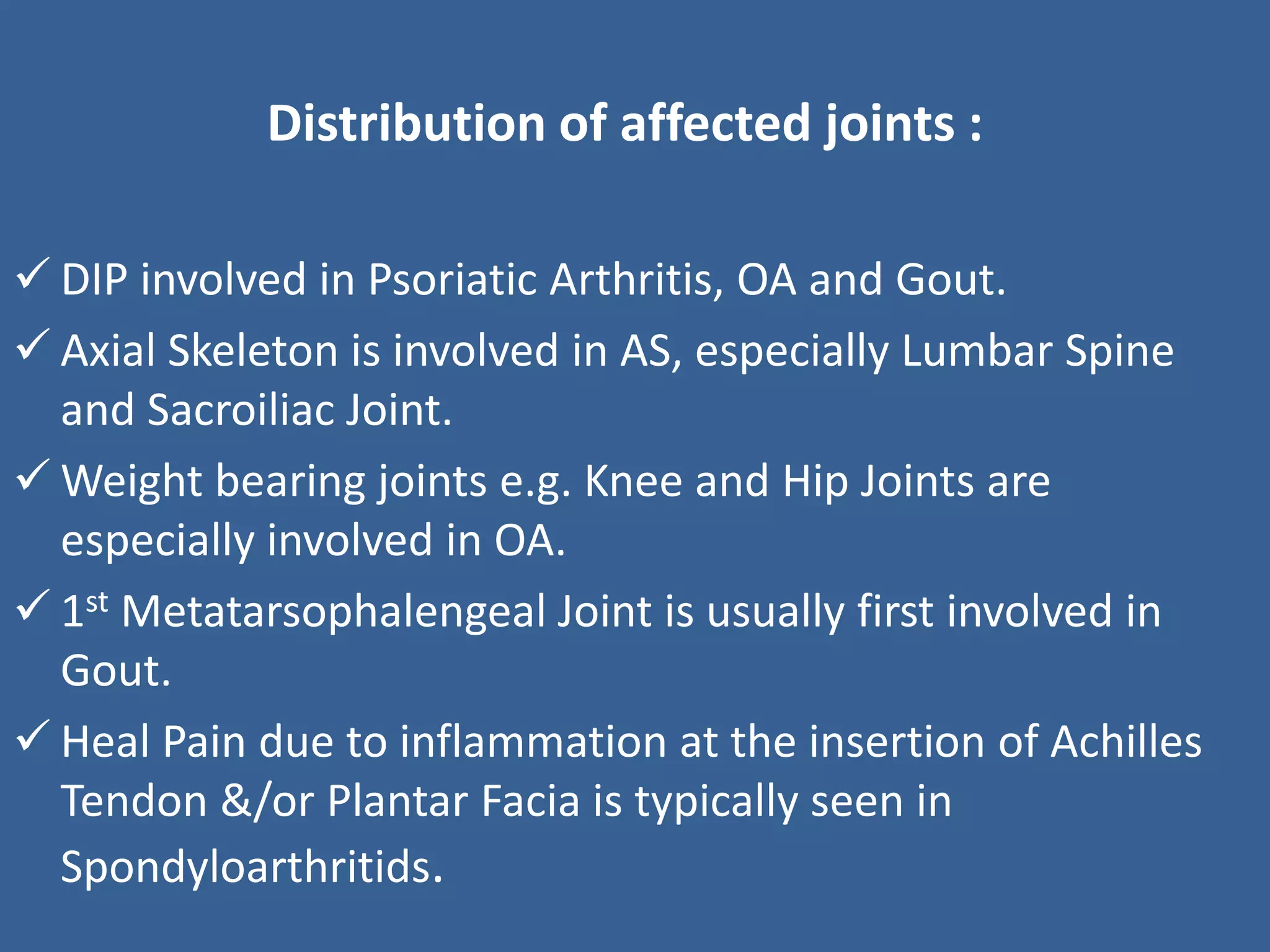
This document provides an overview of how to approach a patient with arthritis. It describes common symptoms of arthritis and how to differentiate between inflammatory and non-inflammatory types based on history, physical exam findings, pattern of joint involvement, onset and duration of symptoms, and additional features. It discusses specific types of arthritis like osteoarthritis, gout, pseudogout, septic arthritis, rheumatoid arthritis, seronegative spondyloarthritides, and others. It provides guidance on diagnostic tests, imaging, and treatment approaches for different arthritis conditions.












![Systemic Lupus Erythematosus
- Characterized by Immune Complex Deposition
involving many organ system.
-Malar rash, Discoid rash, Photosensitivity.
-Oral ulcers, Serositis, Arthritis(non erosive arthritis).
-Renal, Neurological and Hematological Disorders.
-ANA, Immunological Disorder(Anti-DsDNA[70%], Anti-Sm
Ab[25%]).
-Intermittent Polyarthritis.](https://image.slidesharecdn.com/lw4lqy8rb68tqgfngmzg-signature-decc3efa5cbd2dfb64acc0203966ef9898e374da3cce88d13804b8075f737277-poli-180511191202/75/Approach-to-arthritis-26-2048.jpg)








![[Int. med] approach to joint pain from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/064ftjyatacrqjgurlzo-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171713-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)