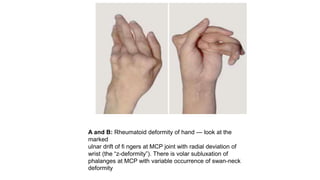
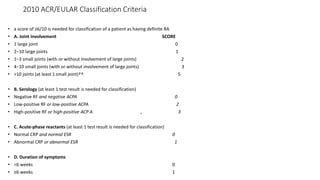
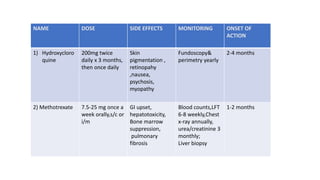
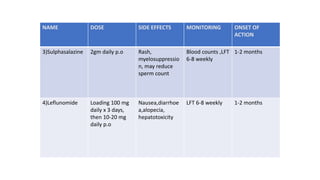
Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by symmetrical inflammatory polyarthritis, primarily affecting the small joints and more common in women. Diagnosis involves clinical symptoms, laboratory findings such as anti-CCP antibodies, and imaging studies to detect joint damage. Management focuses on pain relief, disease modification through DMARDs, and may include biologic therapies, with a need for patient education and individualized treatment plans.




![[Previously Called Second Line Agents (They Are Now the
First Line Agents), Slow-acting Antirheumatic Drugs]—Now
Th ey Are Called “Synthetic” DMARDs (in View of
Availability
of Biological Agents)](https://image.slidesharecdn.com/rheumatoidarthritis-240611044303-c0c446f1/85/RHEUMATOID-ARTHRITIS-with-dmards-classification-pptx-39-320.jpg)





























![AVASCULAR NECROSIS OF FEMORAL HEAD [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/avascularnecrosisoffemoralheadautosaved-250921194430-96361954-thumbnail.jpg?width=640&height=640&fit=bounds)
![CRPS ppt sajad final final [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/crpspptsajadautosaved-250921194258-ec8857be-thumbnail.jpg?width=640&height=640&fit=bounds)




























