This document provides an overview of rheumatoid arthritis (RA). It defines RA as a chronic systemic inflammatory disease that primarily affects the peripheral joints in a symmetrical manner. The usual age of onset is 20-40 years. RA is characterized by chronic synovitis and pannus formation that can erode cartilage and bone. Diagnosis is based on signs and symptoms as well as serological markers like rheumatoid factor. Treatment involves non-pharmacological measures as well as disease-modifying drugs to reduce inflammation and prevent long-term joint damage and disability. Prognosis depends on disease severity, with better outcomes for those who experience early remission.




























![[Int. med] approach to joint pain from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/064ftjyatacrqjgurlzo-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171713-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)





























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

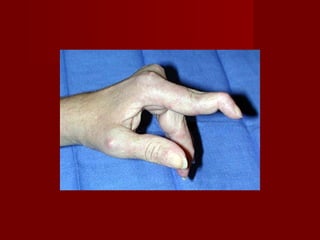
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









