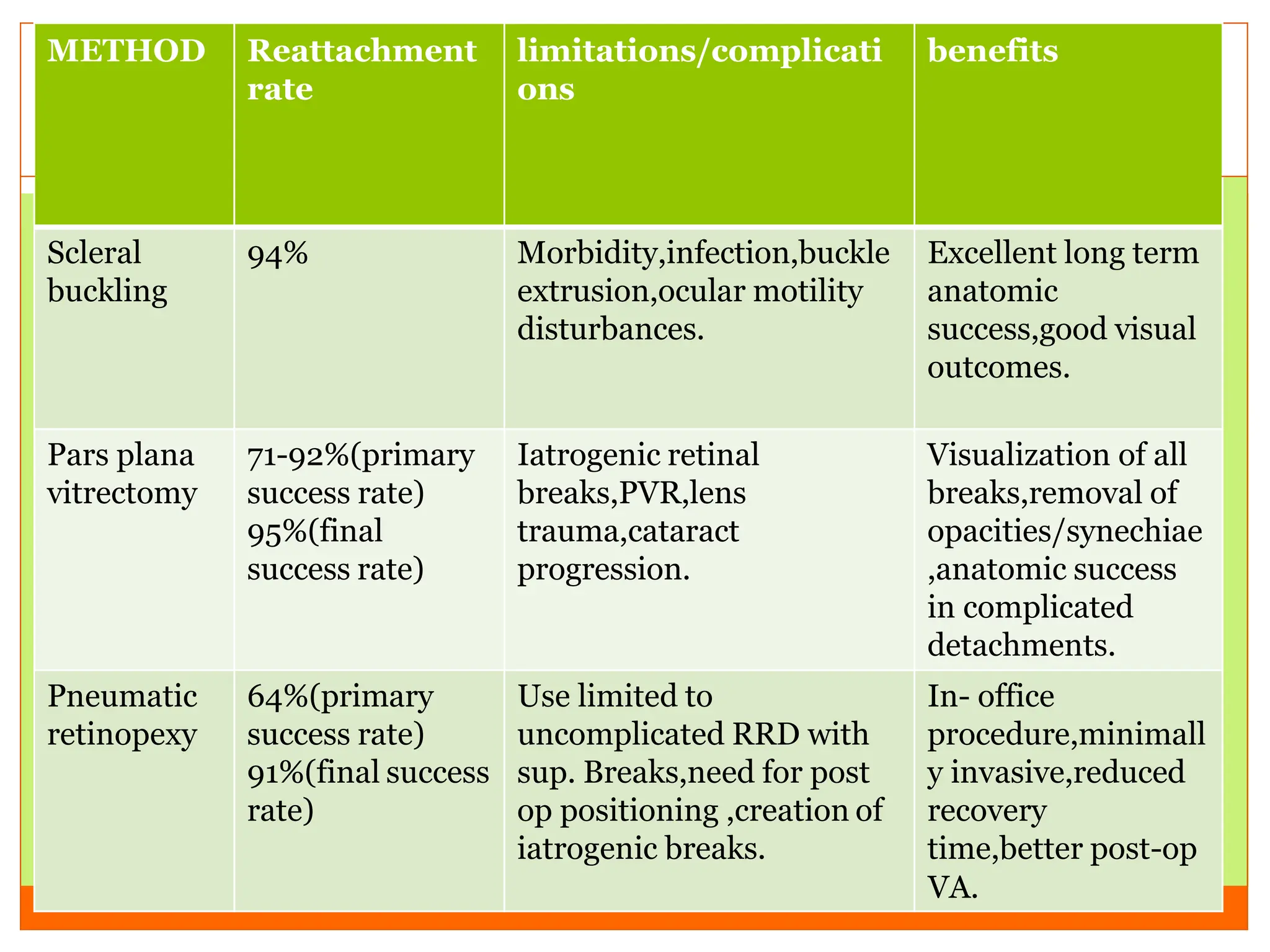
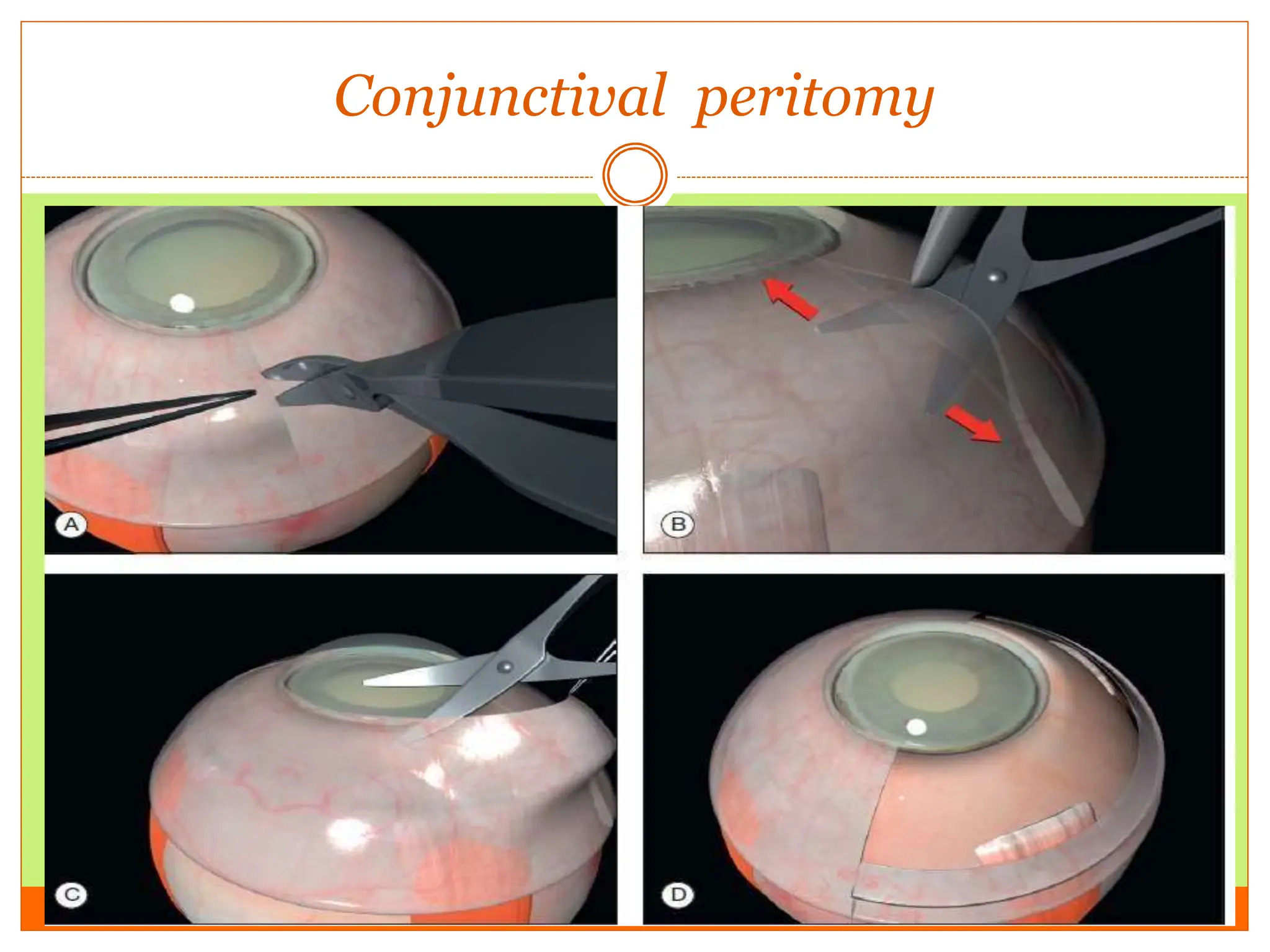
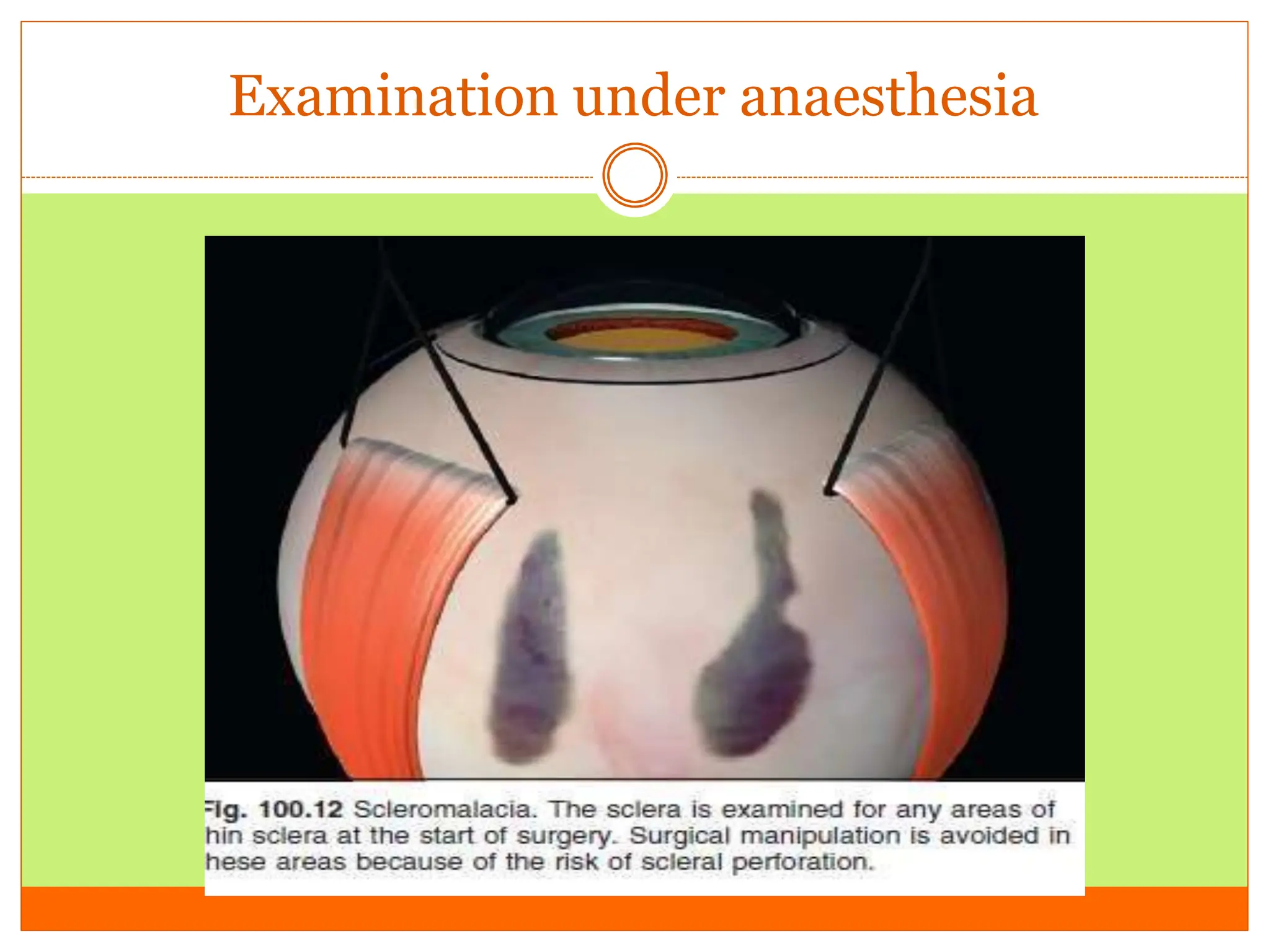
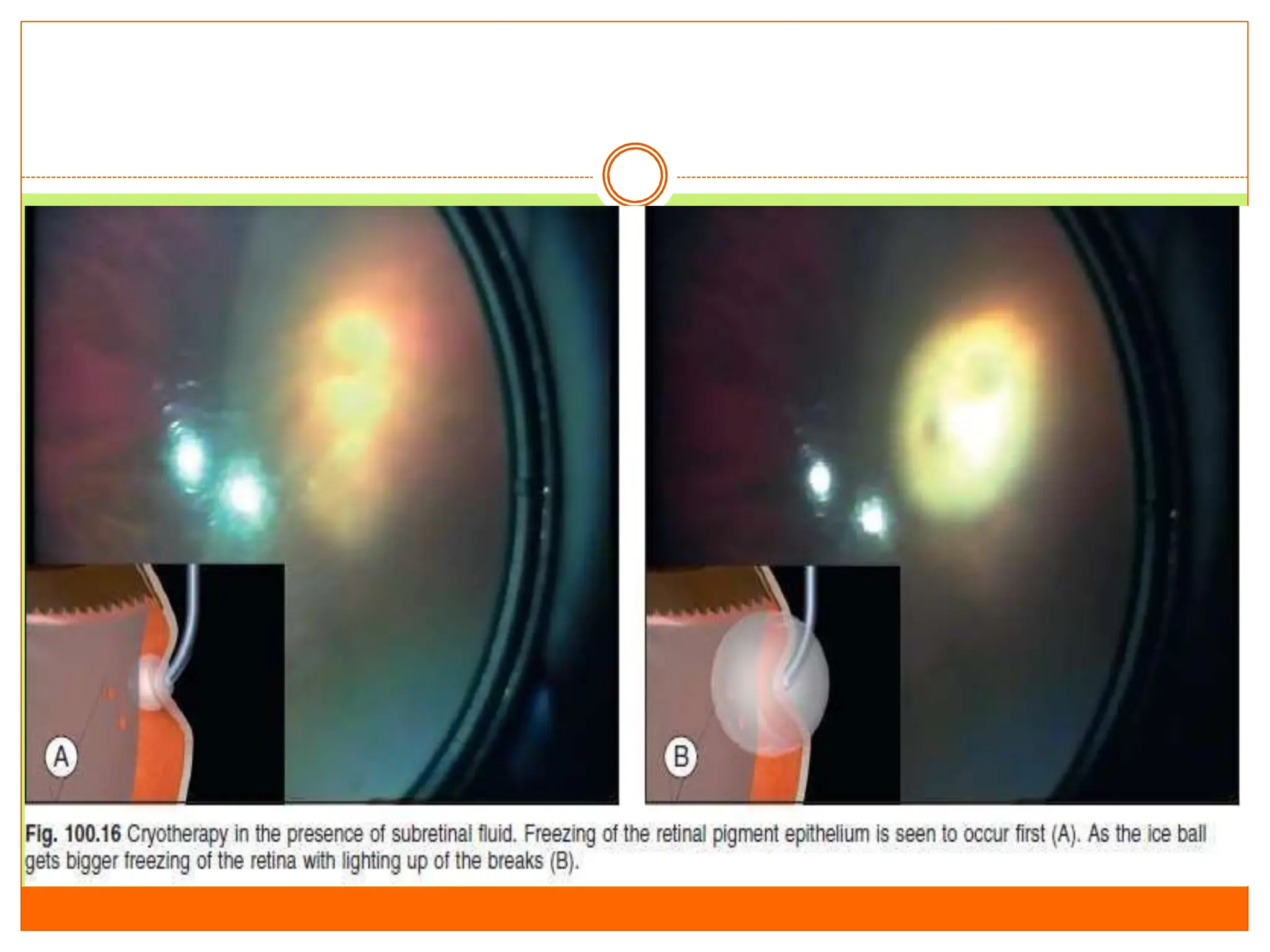
This document provides guidelines for the management of retinal detachment. It discusses various treatment options including scleral buckling, pneumatic retinopexy, and vitrectomy. Scleral buckling involves conjunctival dissection, muscle slinging, cryotherapy or laser retinopexy around retinal breaks, placement of explants or an encircling band, and drainage of subretinal fluid. Pneumatic retinopexy uses an intraocular gas bubble to reattach the retina in cases of uncomplicated retinal detachment from superior breaks. Vitrectomy allows visualization and treatment of all retinal breaks through a pars plana approach using microinstruments under microscope visualization.