Downloaded 191 times
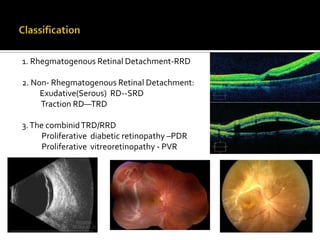
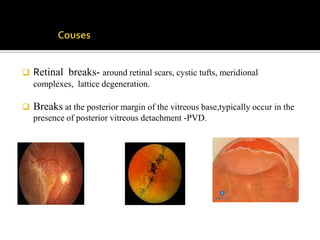
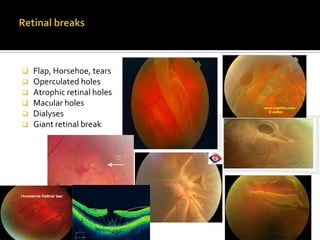
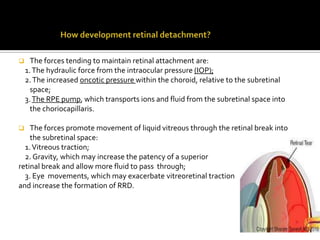
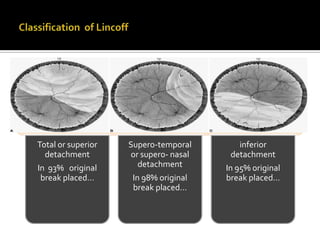
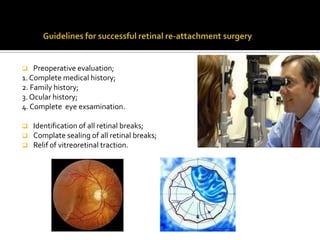
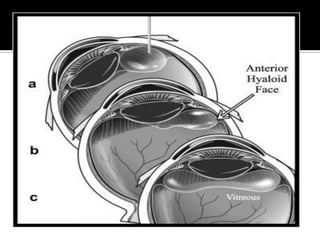
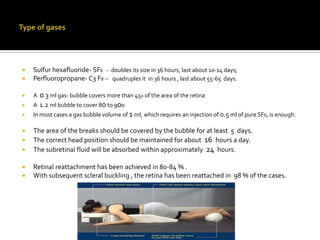
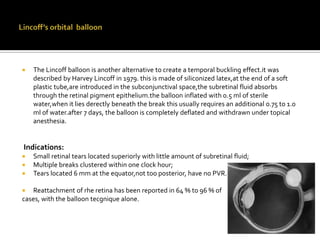



This document discusses retinal detachment, including the different types, causes, evaluation, and surgical treatment options. It covers rhegmatogenous retinal detachment caused by retinal breaks, as well as exudative retinal detachment due to fluid leakage. Surgical techniques mentioned include scleral buckling, pneumatic retinopexy using an expansile gas, vitrectomy, and the use of tamponading agents like gases, silicone oil, and the Lincoff balloon. Complications and failure rates of the procedures are also summarized.


















































































