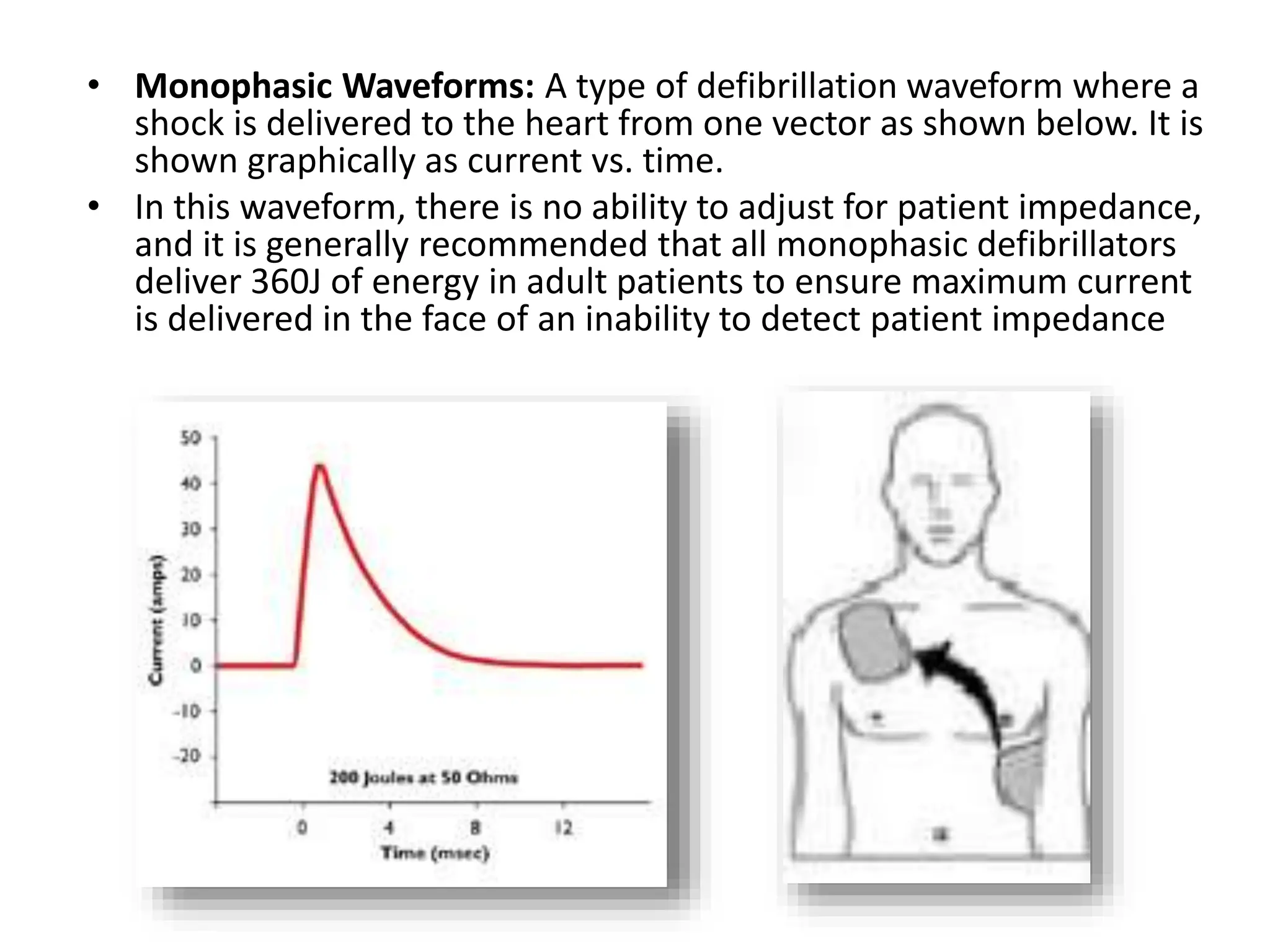
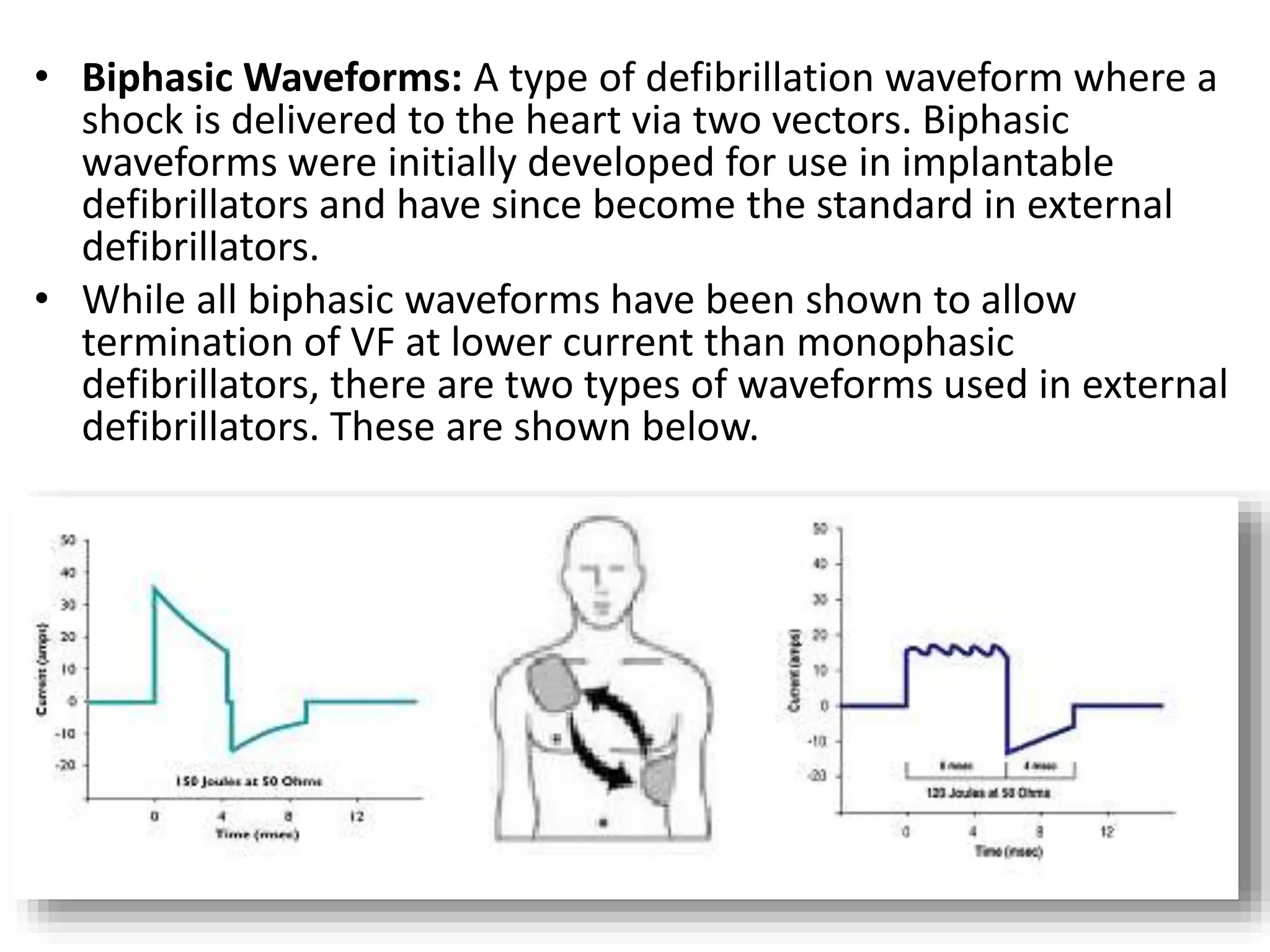
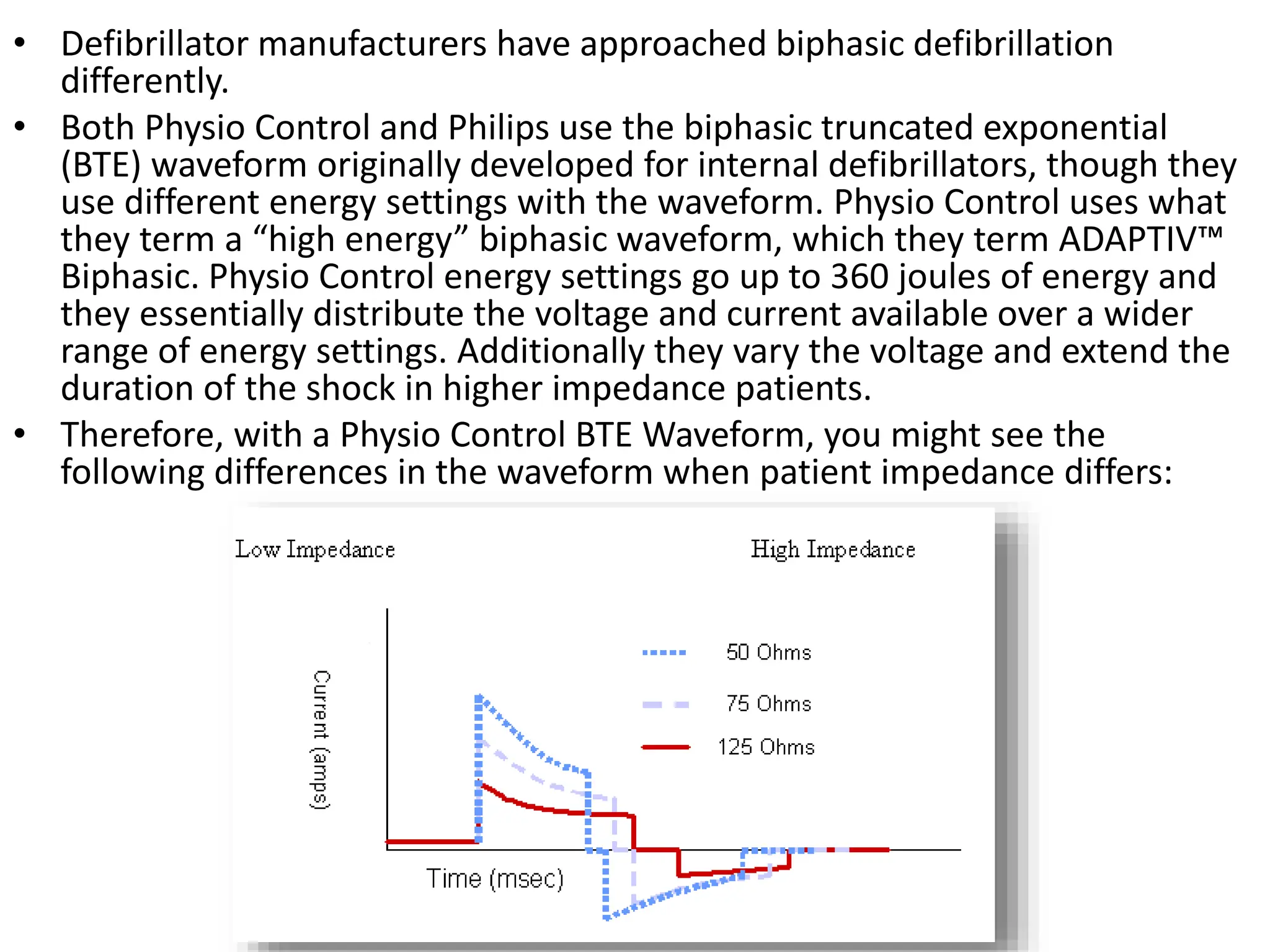
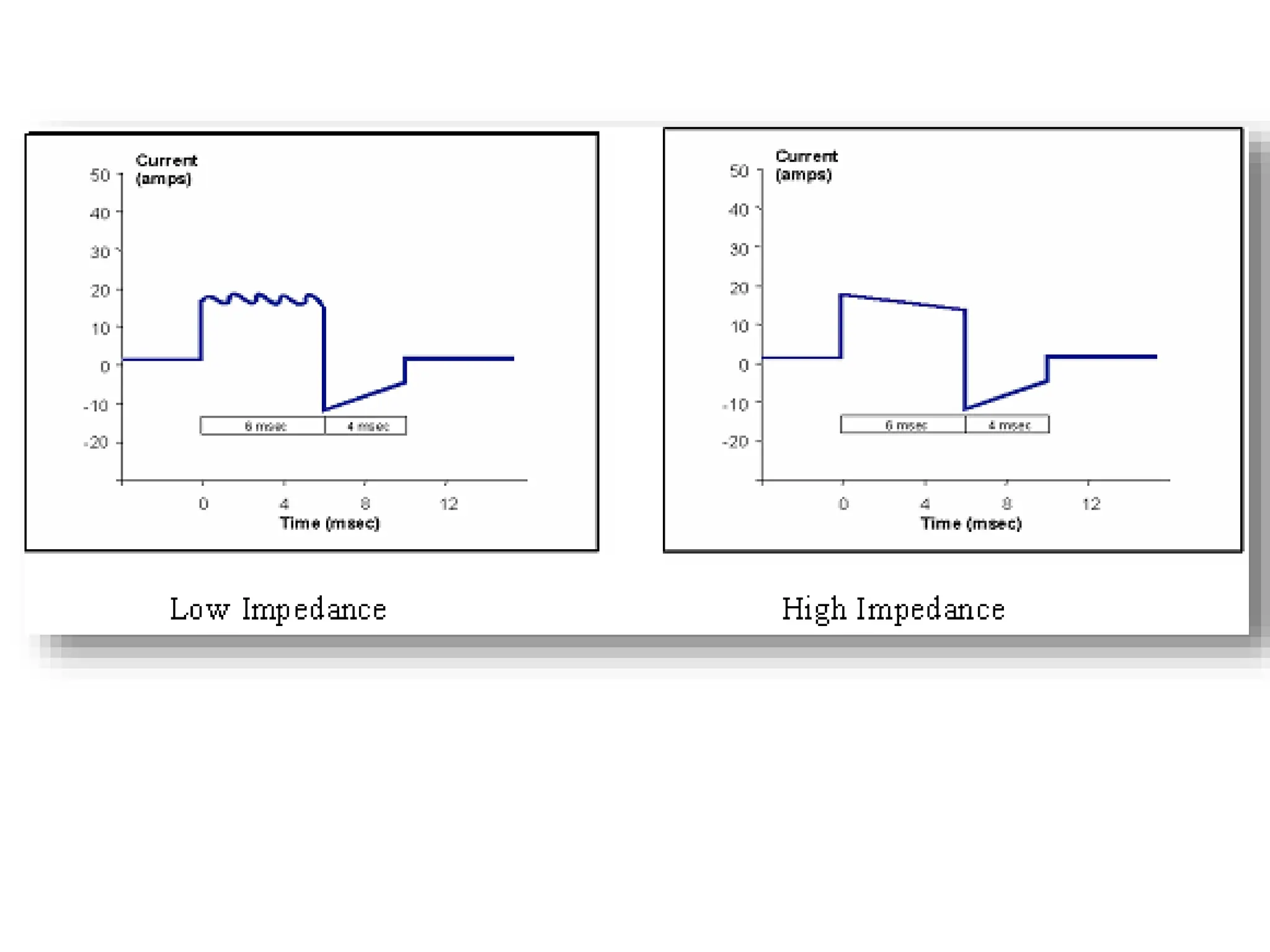
The document discusses the principles and types of defibrillation waveforms, focusing on energy, current, and impedance in defibrillators. It compares monophasic and biphasic waveforms, detailing their characteristics and energy settings used by different manufacturers like Physio Control, Philips, and Zoll Medical. The summary concludes that while various biphasic waveforms exist, none have been proven superior despite clinical trials.

















































![BIOMEDICAL_WASTE_MANAGEMENT[1].pptx 22222.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/biomedicalwastemanagement1-240420050706-3b1ae262-thumbnail.jpg?width=640&height=640&fit=bounds)

























