The document discusses micturition and the urinary system. It describes:
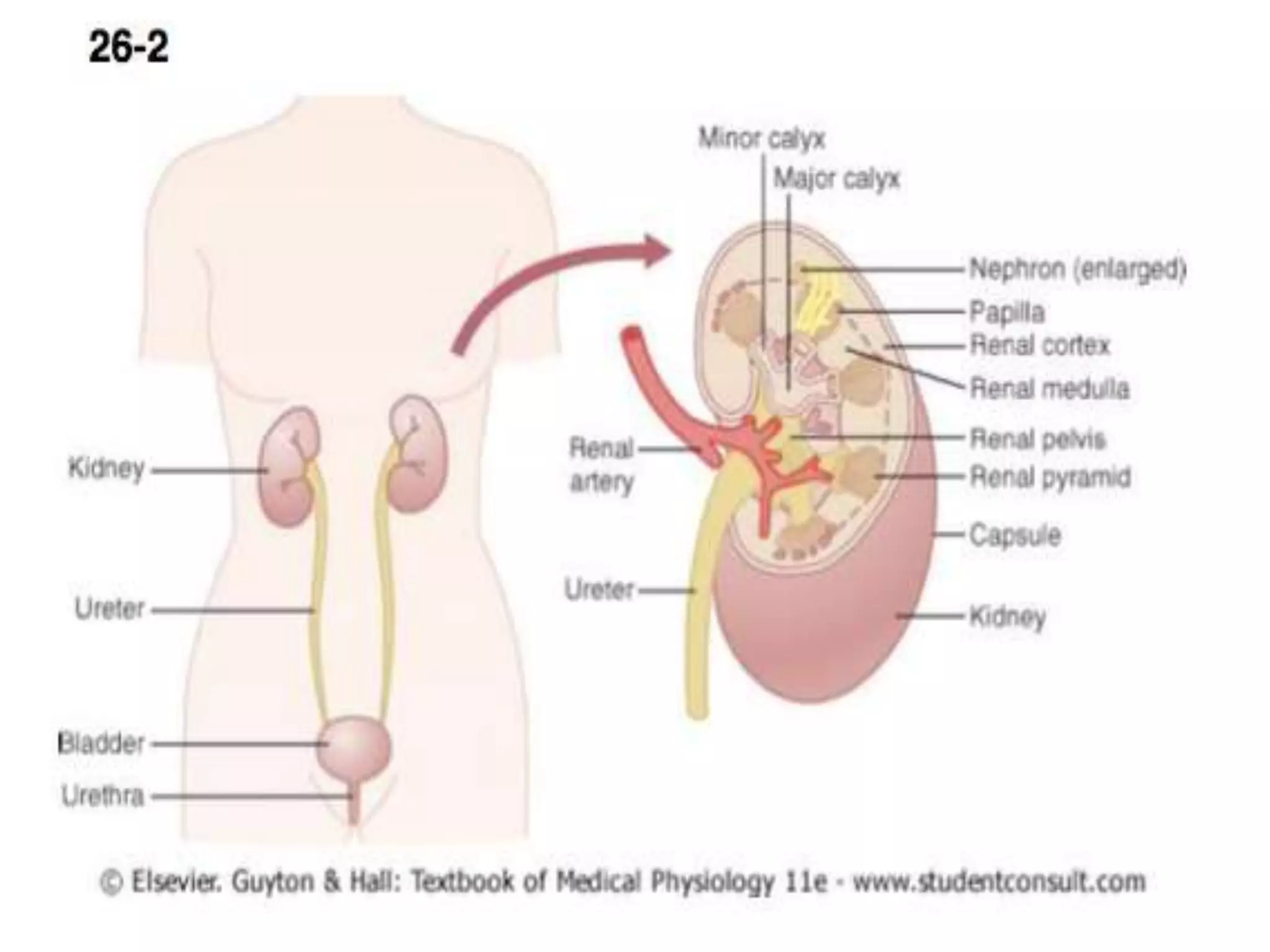
1. The renal system which includes kidneys, ureters, urinary bladder, and urethra.
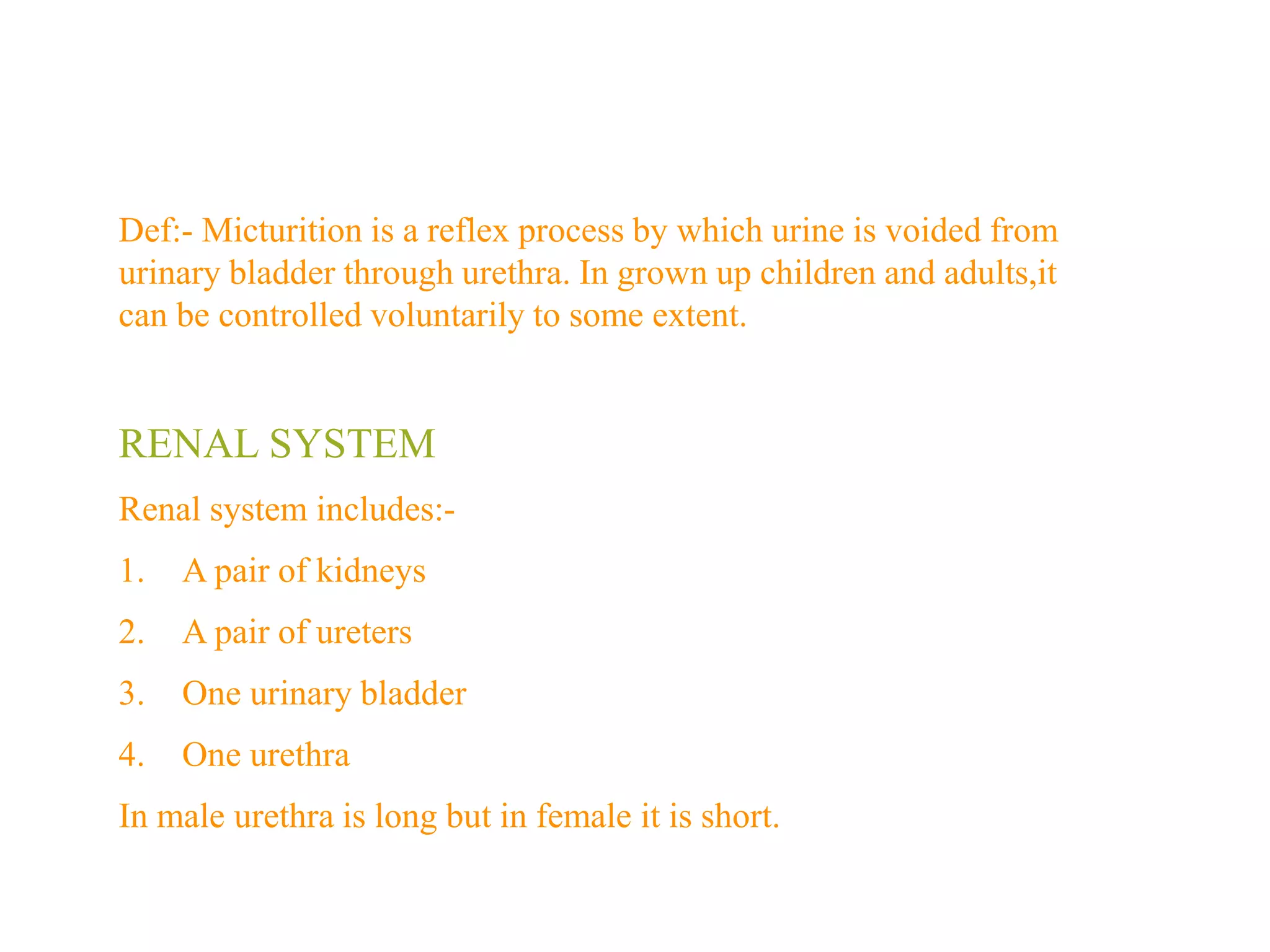
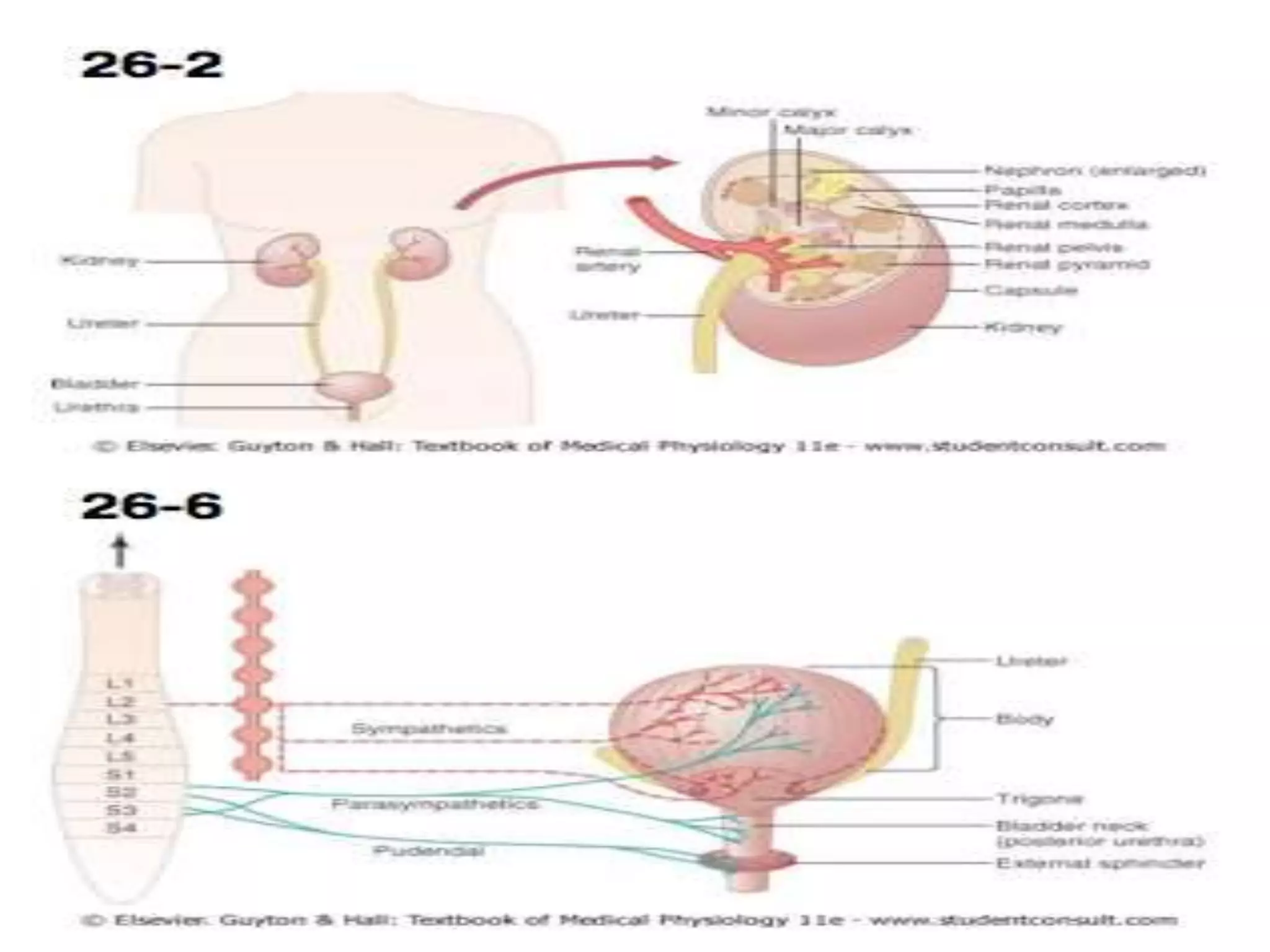
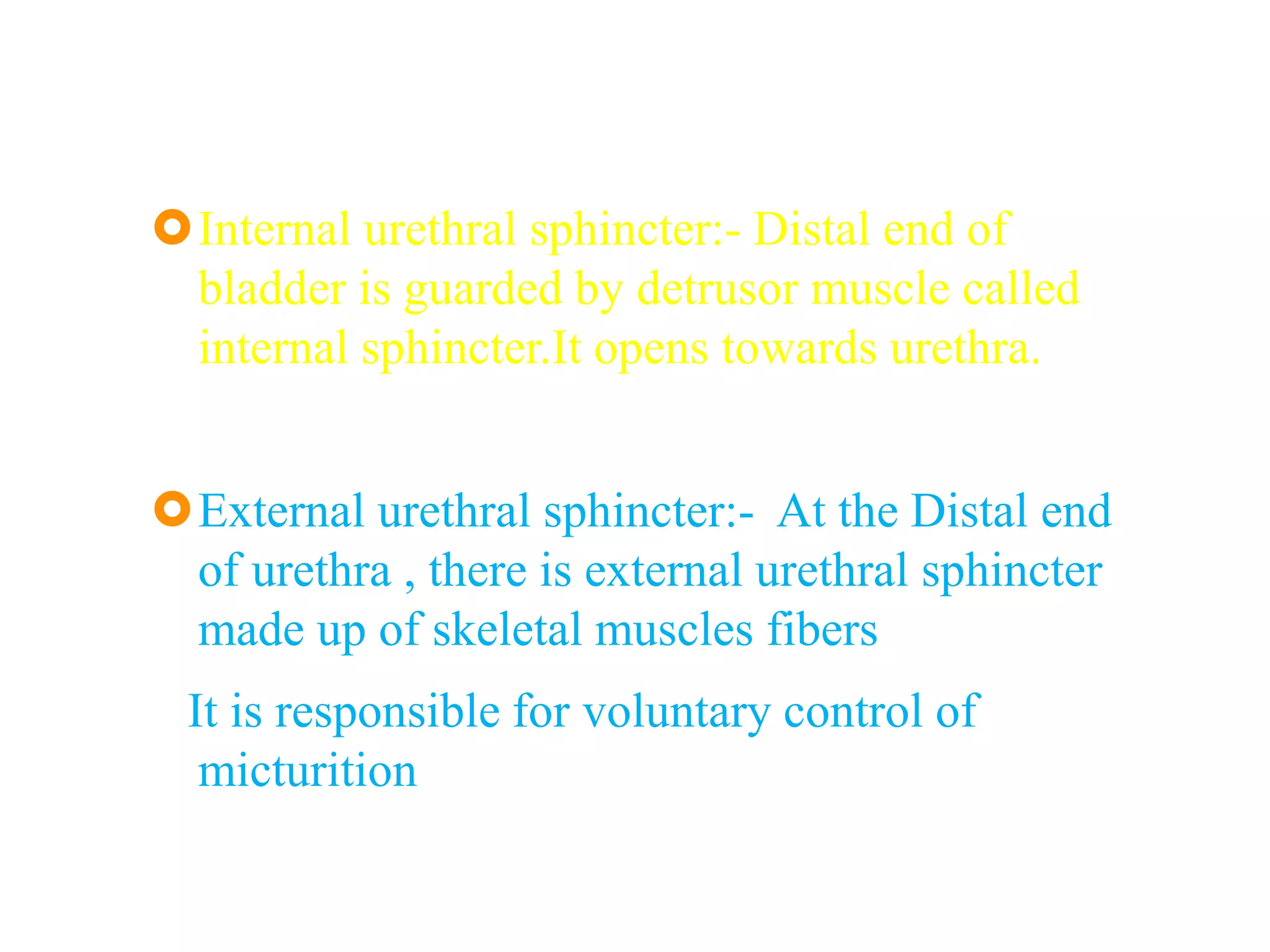
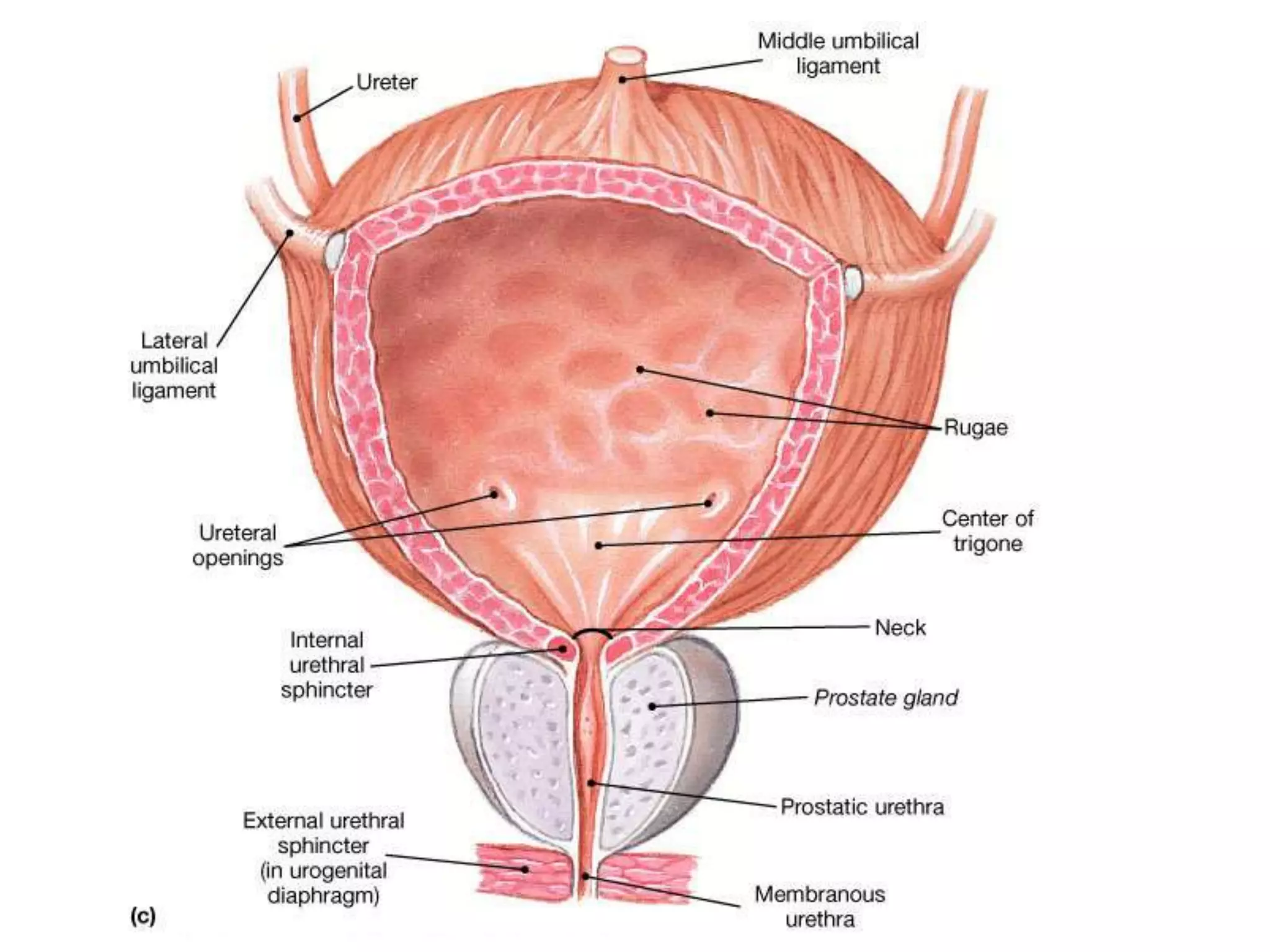
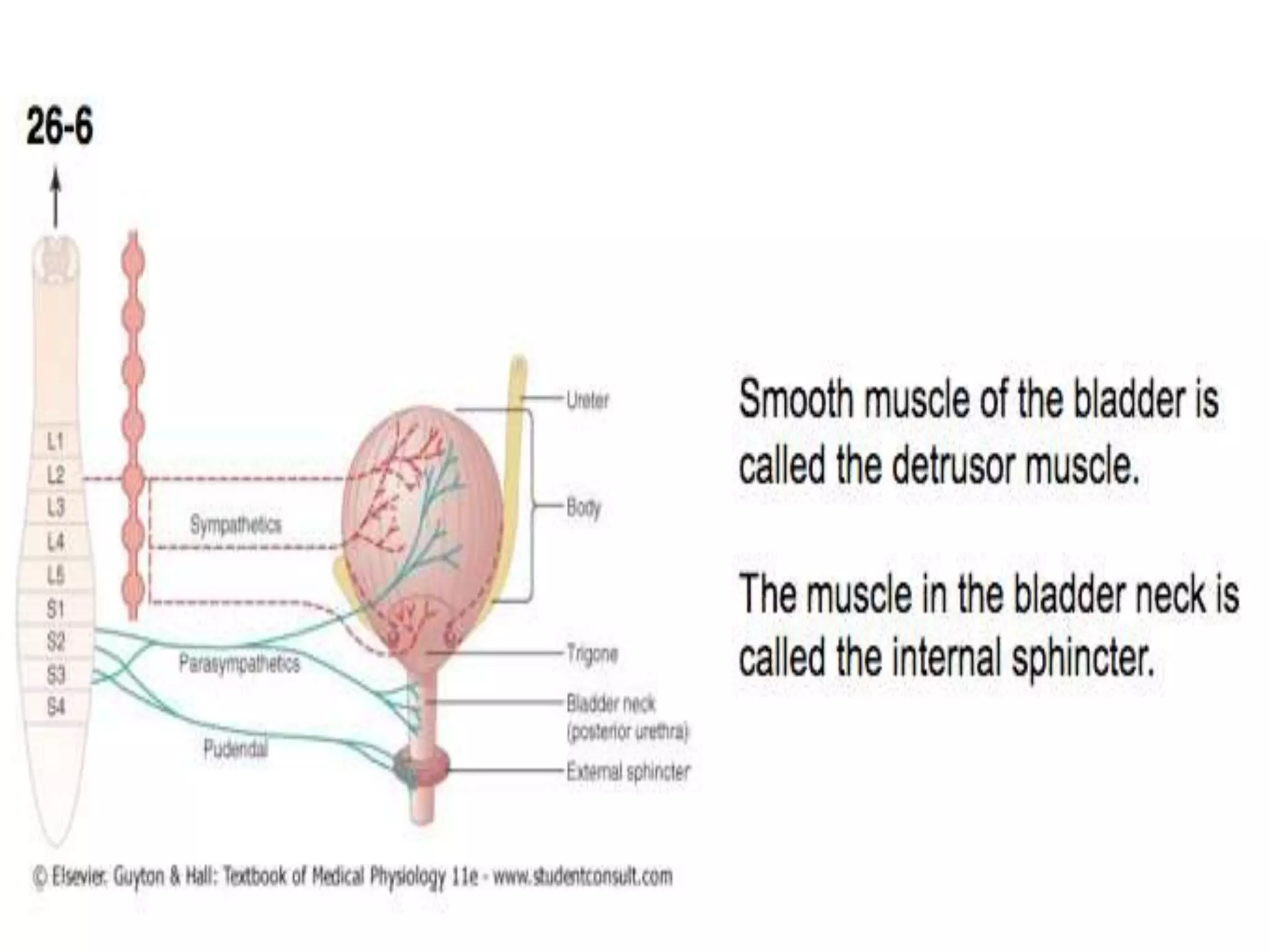
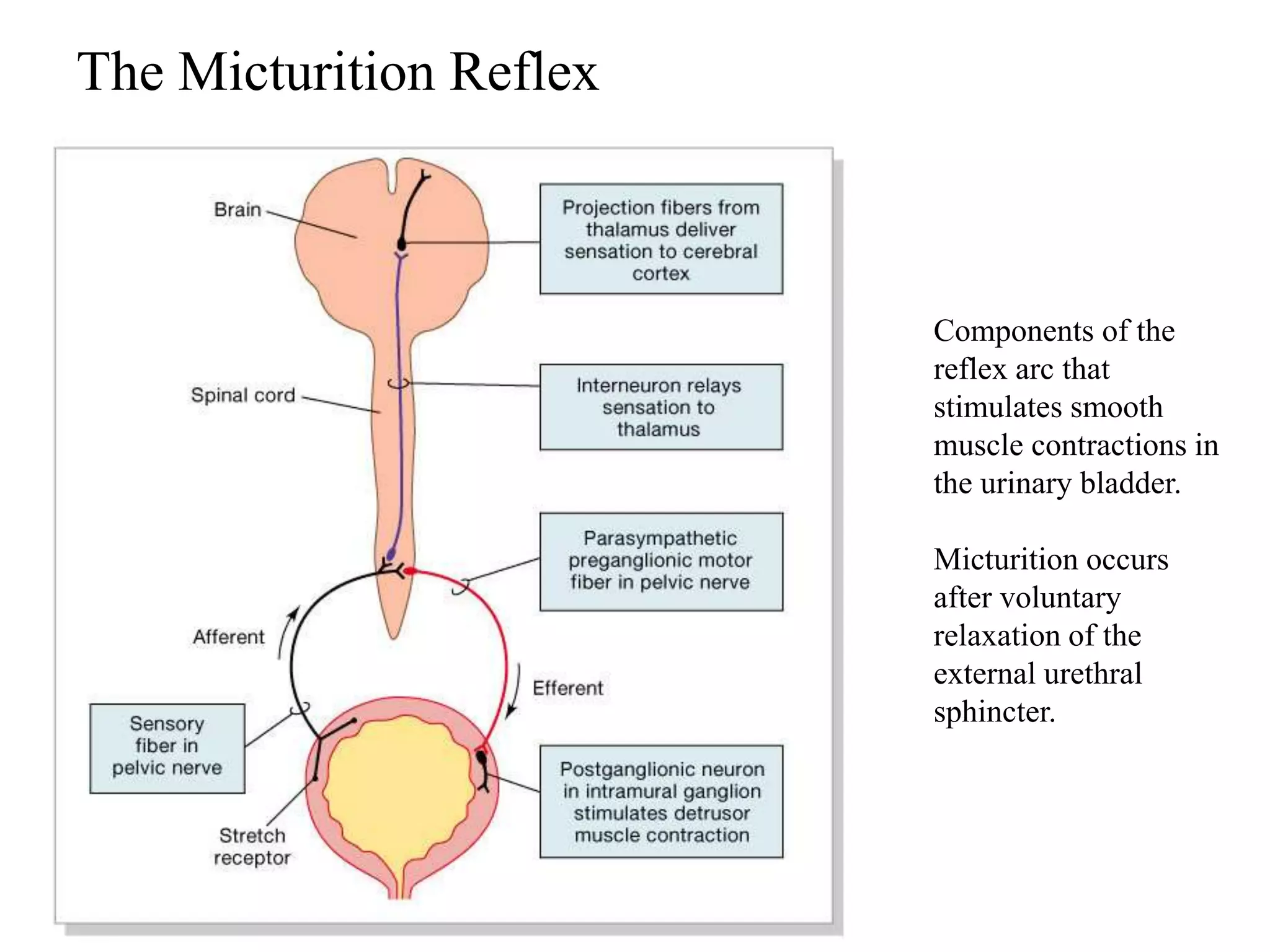
2. The anatomy and nerve supply of the urinary bladder. The bladder is innervated by the sympathetic, parasympathetic, and somatic nervous systems.
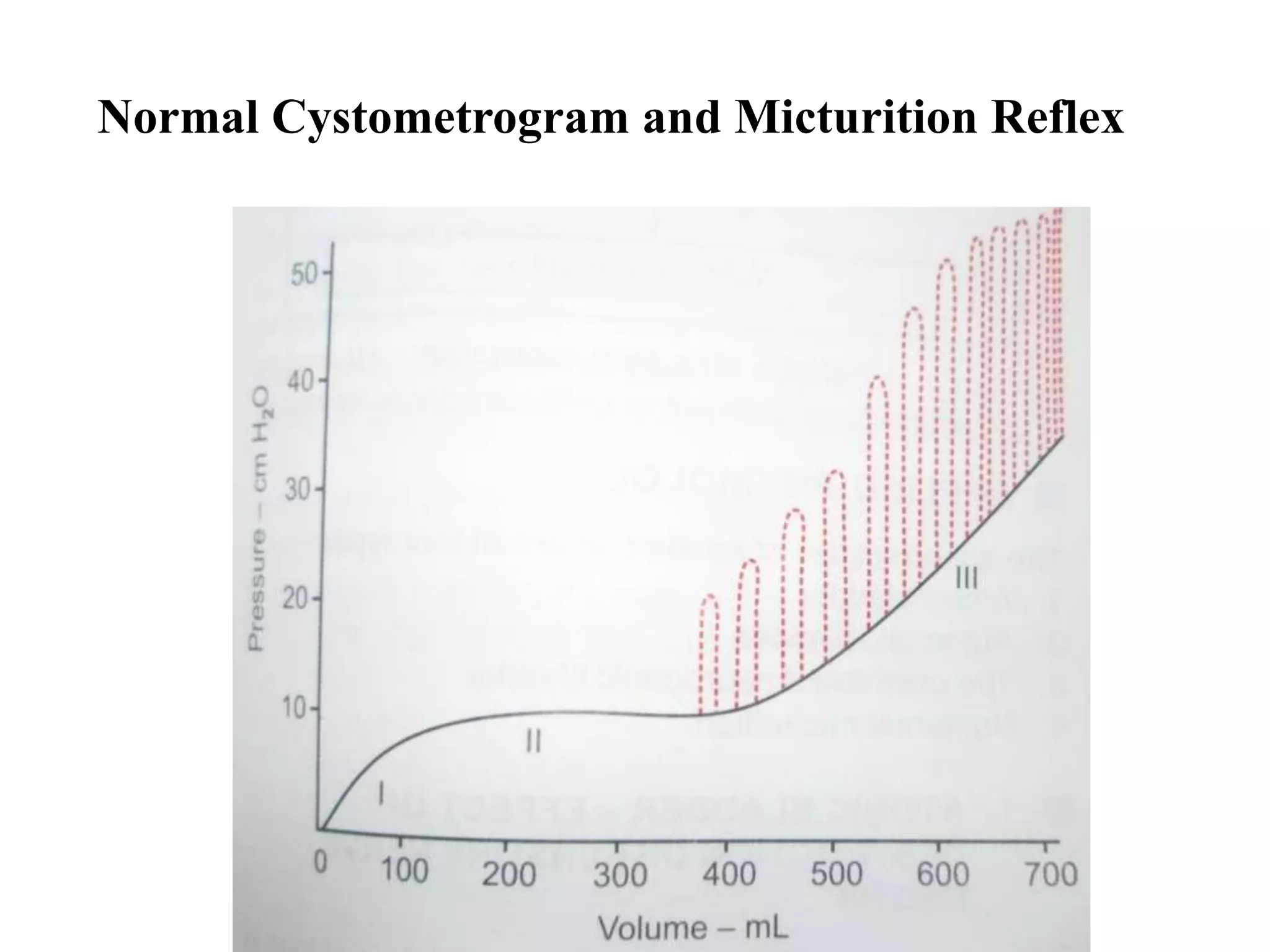
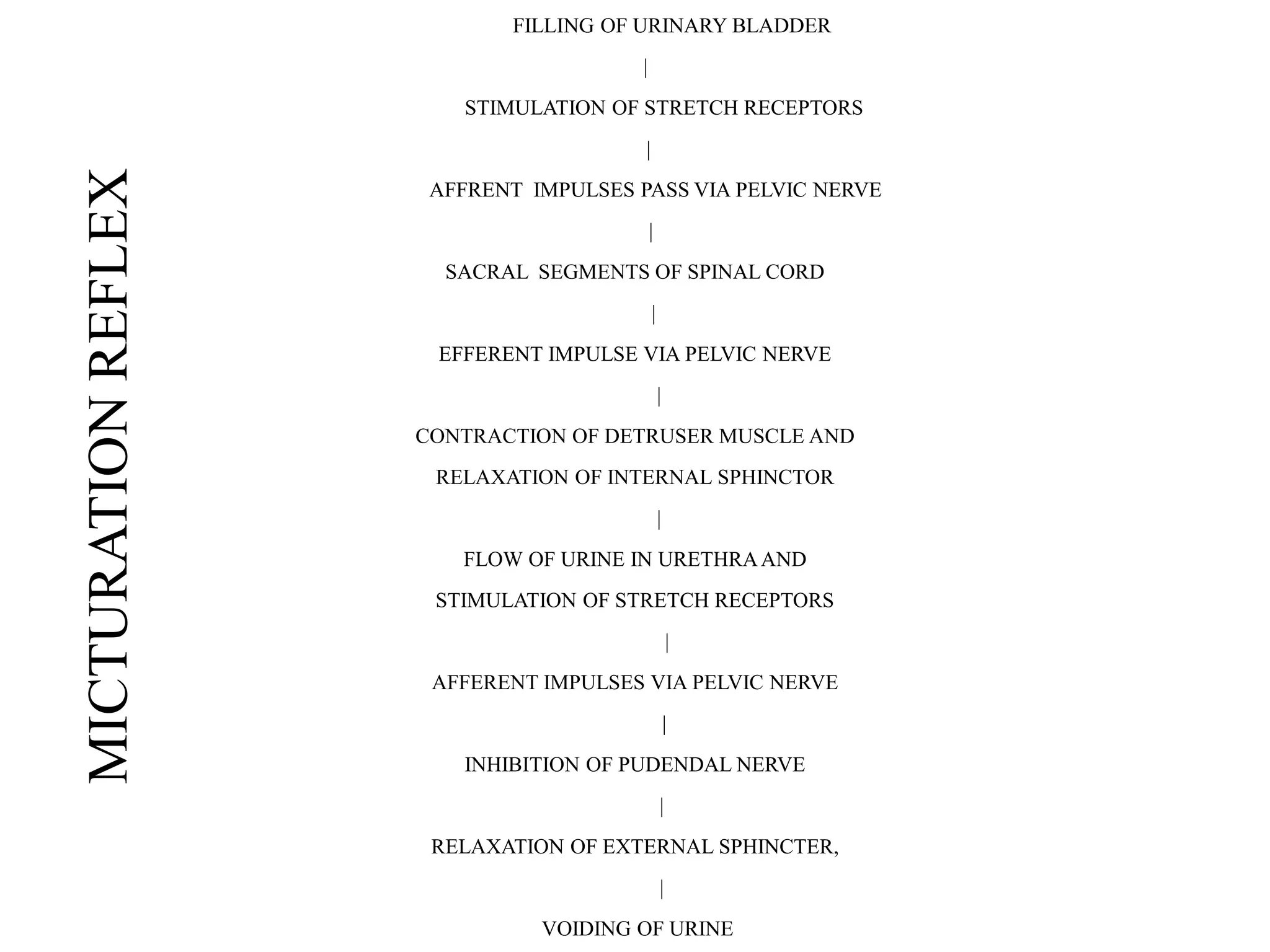
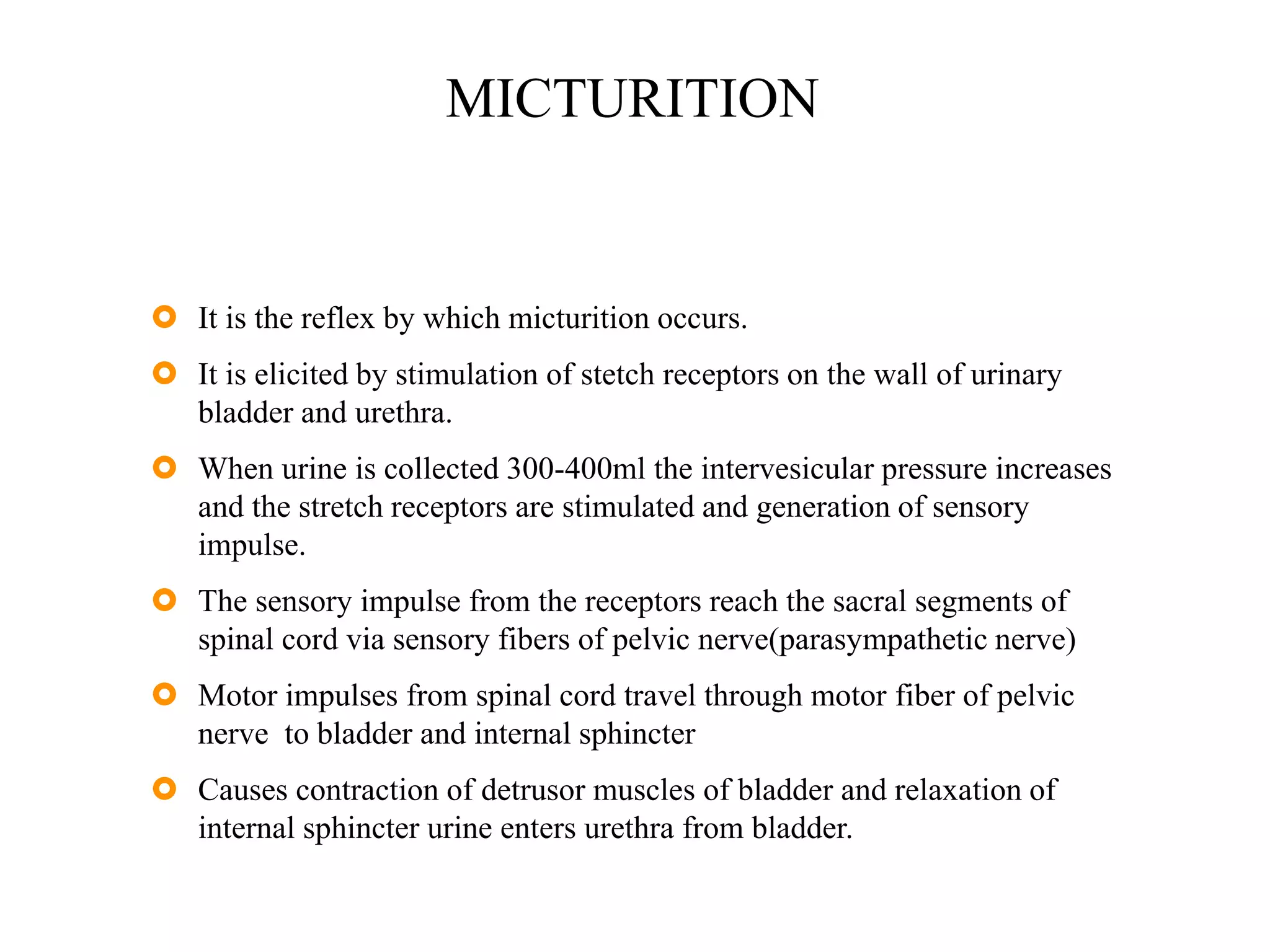
3. The micturition reflex which is triggered by bladder filling and involves contraction of the detrusor muscle and relaxation of the internal urethral sphincter to void urine in a coordinated process.




































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


















