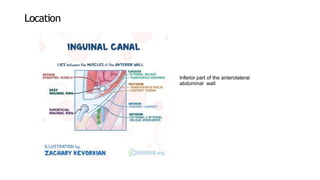
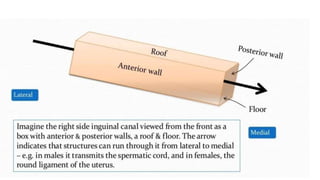
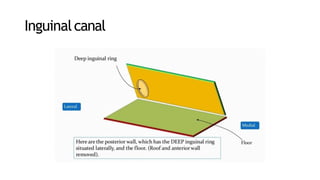
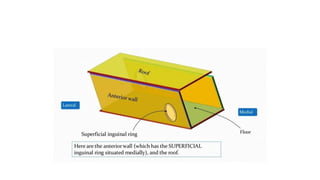
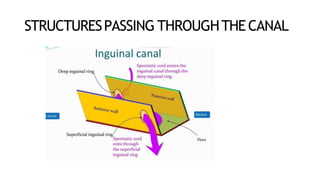
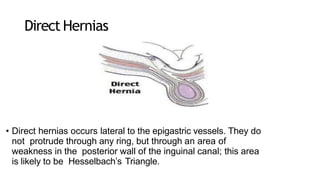
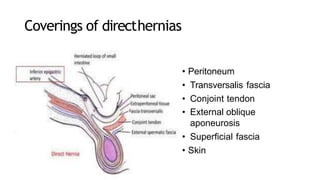
The inguinal canal is a passage in the lower anterior abdominal wall that extends from the deep inguinal ring to the superficial inguinal ring. It is about 4cm long and directed downward and medially. The spermatic cord in males or round ligament in females pass through the canal. The walls of the canal have multiple layers including skin, fascia, and muscles. The canal allows communication between intra-abdominal and scrotal contents while preventing herniation. Mechanisms like the flap valve prevent herniation during increases in intra-abdominal pressure. Direct and indirect inguinal hernias can occur through the canal.