The document discusses various diseases of the iris, including congenital anomalies, inflammations, degeneration, and tumors. Key topics include heterochromia, anterior uveitis, treatment options, and complications arising from iridocyclitis. It also outlines symptoms, signs, and investigative measures related to iris disorders.
![CONTENTS
DISEASE OF IRIS –
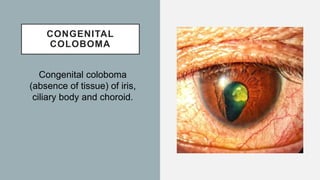
• Congenital Anomalies
• Inflammations [Anterior uveitis]
• Types Of Iridocyclitis
• Degeneration of iris
• Cyst and tumours of iris](https://image.slidesharecdn.com/diseasesofiris-231122051926-aa5d7b00/85/DISEASES-OF-IRIS-pptx-2-320.jpg)
![CONGENITAL ANOMALIES
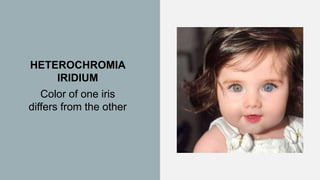
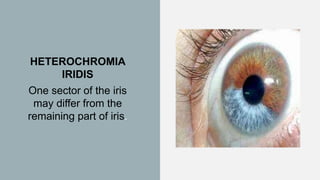
HETEROCHROMIA OF IRIS
Heterochromia is a variation in coloration most often used to
describe color differences of the iris, but can also be applied to
color variation of hair[1] or skin.
In heterochromia iridium, color of one iris differs from the other.
In heterochromia iridis, one sector of the iris may differ from the
remainder of iris.](https://image.slidesharecdn.com/diseasesofiris-231122051926-aa5d7b00/85/DISEASES-OF-IRIS-pptx-4-320.jpg)
![POLYCORIA
Polycoria is a pathological
condition of
the eye characterized by more
than one pupillary opening in
the iris.[1]](https://image.slidesharecdn.com/diseasesofiris-231122051926-aa5d7b00/85/DISEASES-OF-IRIS-pptx-7-320.jpg)

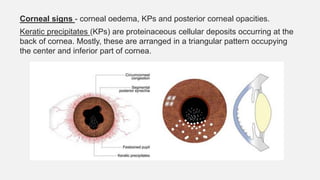

![Iris signs -
Loss of normal pattern - occurs due to oedema.
Changes in iris colour due to hyperpigmentation and
depigmentation.
Posterior synechiae - adhesions b/w posterior surface of iris &
anterior part of lens.
Pupillary signs –
Narrow pupil - due to irritation of sphincter pupillae by toxins.
Irregular pupil shape - results from segmental posterior synechiae
formation. [festooned pupil]
Pupillary reaction becomes sluggish or absent due to oedema and
hyperaemia of iris.](https://image.slidesharecdn.com/diseasesofiris-231122051926-aa5d7b00/85/DISEASES-OF-IRIS-pptx-16-320.jpg)