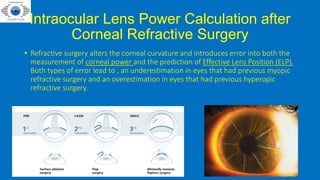
The document presents an extensive overview of intraocular lens (IOL) power calculations, particularly in special cases such as post-refractive surgery and pediatric applications. It discusses various methodologies and formulas for accurate IOL power determination, emphasizing the complications arising from surgical history like keratometry errors. The text also outlines guidelines for specific populations, including those with corneal transplants and post-vitrectomized eyes, to improve surgical outcomes.

![Indirect Method
1. Clinical history method : The corneal power is calculated by
Corneal power before refractive surgery - Change in manifest refraction at the
corneal plane
Convert the pre and postoperative refraction into Spherical Equivalent Refraction.
Now convert this SER at spectacle plane to SER at corneal plane .
SEQC=1000/[(1000/SEQS)-Vertex Distance]
Unavailability or inaccuracy of these data and interval changes in the corneal
curvature or lens power pose a problem .
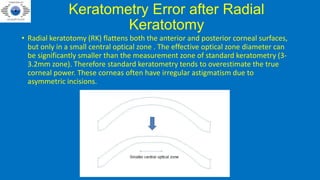
Also, clinical history method is not suitable for RK because of unstable corneal
power (Post RK cornea typically flattens progressively over many years).](https://image.slidesharecdn.com/iolpowerinlasiksiliconepeds-220717071940-e3e7351f/85/IOL-CALCULATIONS-IN-SPECIAL-CASES-9-320.jpg)