Downloaded 36 times














![17
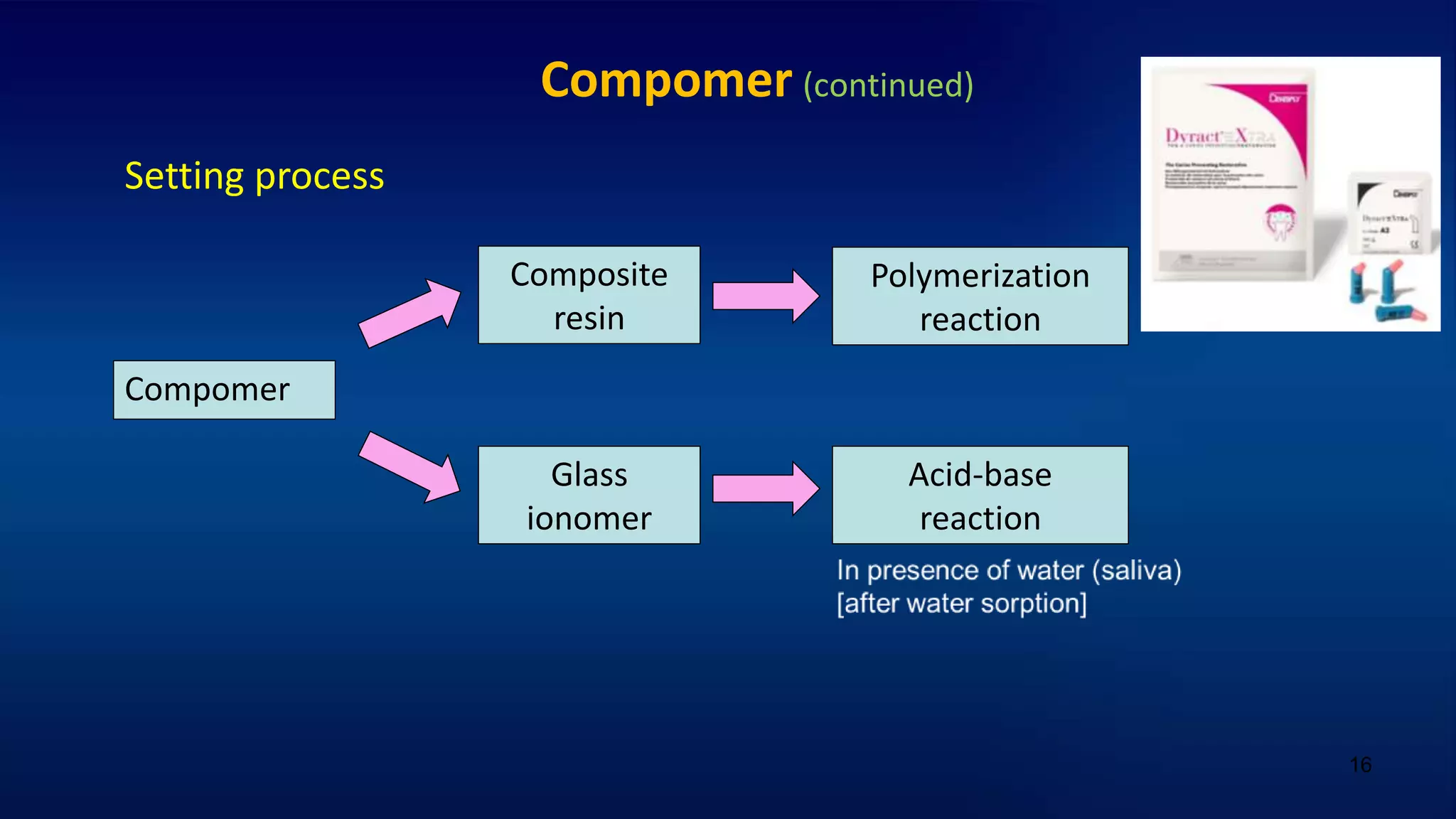
Compomer (continued)
Disadvantages
1- Fl release: lower than glass ionomer (10% of that released by glass ionomer)
- Lower amount & duration of Fl release
- No recharge from fluoride treatment [Textbook: Craig 14 ed 2019]
2- Bond: still needs etching & dentin bonding agent prior to its placement
3- Esthetic: lower than composite resin.
- Lower color stability: due to change in refractive index by
water absorption & staining [Textbook: Phillips 12 ed 2013]
4- Wear resistance: lower than composite resin](https://image.slidesharecdn.com/manchesterrecentcomposites-210516120828/75/Recent-dental-composite-resins-17-2048.jpg)

![19
GIOMER (PRG) [continued]
Indications (uses)
Restoration (filling) of root caries
Class III & V cavities
Advantages
1- Fl release & recharge
2- Biocompatible
3- Excellent esthetic
& smooth surface finish](https://image.slidesharecdn.com/manchesterrecentcomposites-210516120828/75/Recent-dental-composite-resins-19-2048.jpg)
![20
Flowable composite
Flowable = has high flow …… Why??
Low filler loading (50%) →
* ↓ viscosity & ↑ flow → [ Pit & fissure sealant ]
* ↓ modulus of elasticity & ↑ flexibility →
stress breaker (absorb stresses) → [ Liner under class I & II ]
* ↓ mechanical properties → [ Non stress-bearing areas ]
* ↑ resin amount → ↑ polymerization shrinkage](https://image.slidesharecdn.com/manchesterrecentcomposites-210516120828/75/Recent-dental-composite-resins-20-2048.jpg)





























Recent advances have improved dental composite materials. Composites contain resin and inorganic fillers to increase strength while decreasing problems from resin such as shrinkage. Larger filler particles improve strength but smoothness while smaller fillers enhance esthetics. Novel composites aim to reduce shrinkage through techniques like silorane resin which uses a different polymerization or bulk fill which can be placed in 4mm layers. Other trends include nano-filled composites with ultra-small particles achieving high filler loading and strength, and smart composites which release ions to prevent decay. Indirect composites can be contoured outside the mouth but still experience shrinkage during cementation. Overall composites continue advancing but shrinkage remains a challenge.





![RECENT ADVANCES AND DEVELOPMENTS IN COMPOSITE DENTAL RESTORATIVE [Autosaved]....](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancesanddevelopmentsincompositedentalrestorativeautosaved-220719151352-01a90a41-thumbnail.jpg?width=640&height=640&fit=bounds)













































































