Downloaded 951 times





























































![ Launched in 1995 by Heraeus-kulzer
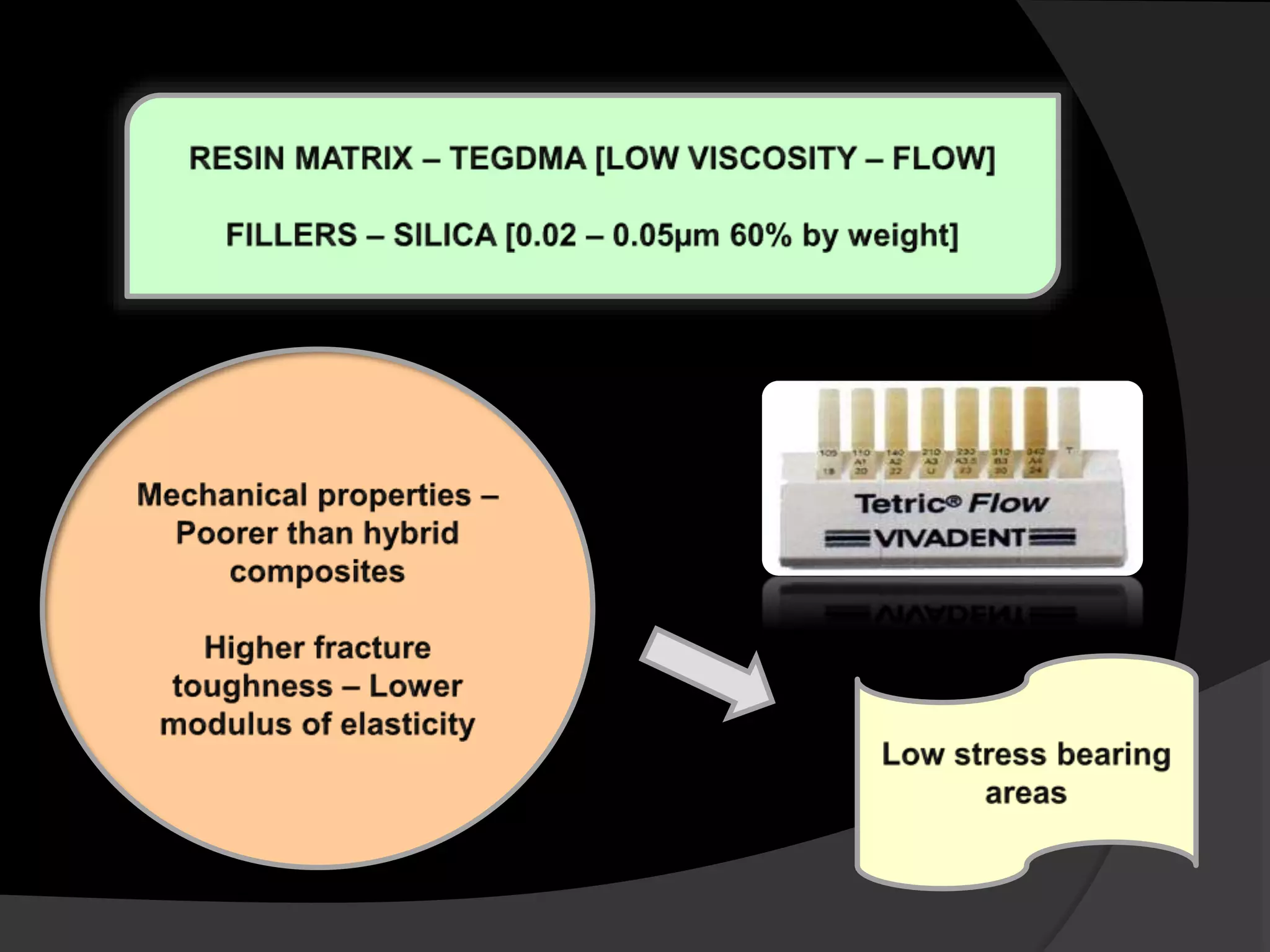
MATRIX FILLER
Organic resin matrix
[BisGMA / UDMA]
Barium silicate glass
0.7µ](https://image.slidesharecdn.com/trendsincompositedentistry-171101181343/75/Recent-advances-in-composite-dentistry-82-2048.jpg)








































The document reviews advancements in aesthetic and restorative dentistry, focusing on composite materials used for dental repairs and enhancements. It discusses various types of composites, their applications, properties, and innovative technologies like nanocomposites and smart composites. Furthermore, it emphasizes the ongoing potential for improvement in resin-based dental materials through advancements in material science and technology.


![RECENT ADVANCES AND DEVELOPMENTS IN COMPOSITE DENTAL RESTORATIVE [Autosaved]....](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancesanddevelopmentsincompositedentalrestorativeautosaved-220719151352-01a90a41-thumbnail.jpg?width=640&height=640&fit=bounds)
































































