



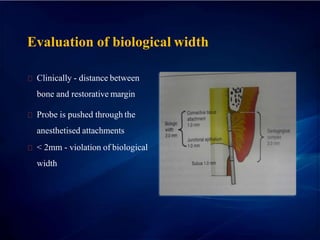













The document outlines various techniques and materials for gingival retraction, essential for making accurate dental impressions. It categorizes retraction methods into mechanical, chemical-mechanical, and surgical and discusses the importance of selecting appropriate materials to avoid gum damage and ensure patient comfort. Additionally, it addresses the biological considerations regarding gingival anatomy, margin placement, and the implications of retraction procedures on oral health.



























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







