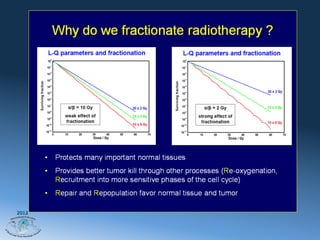
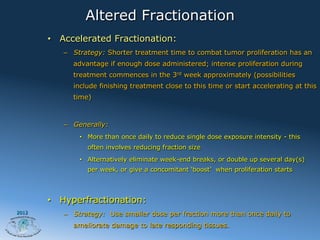
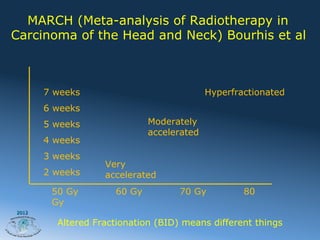
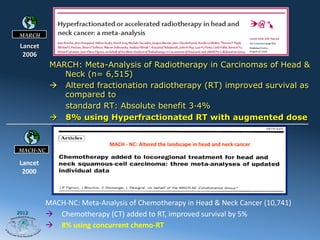
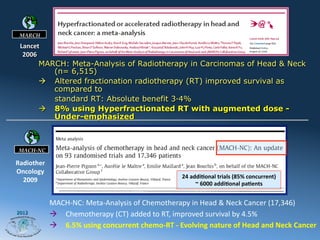
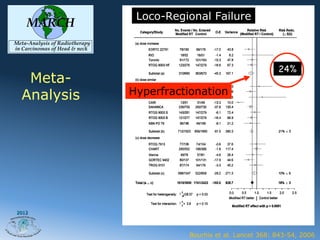
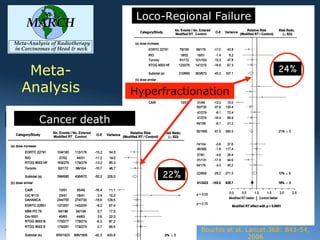
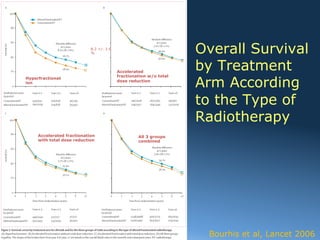
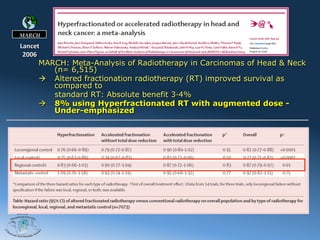
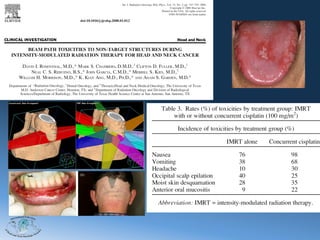
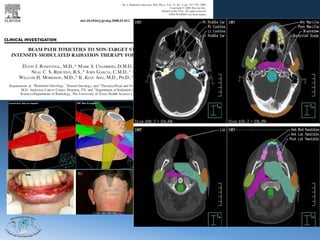
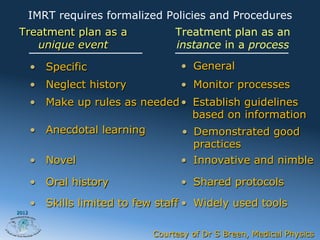
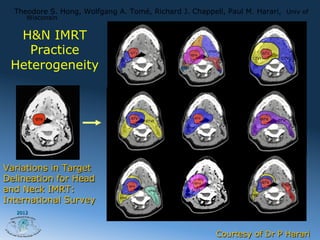
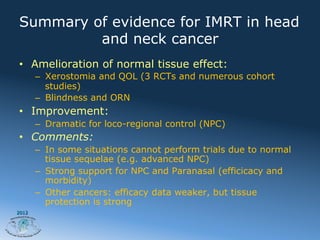
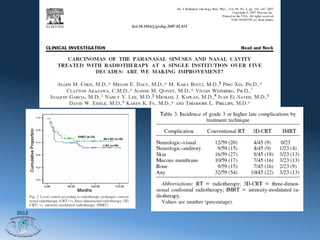
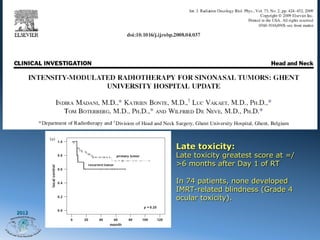

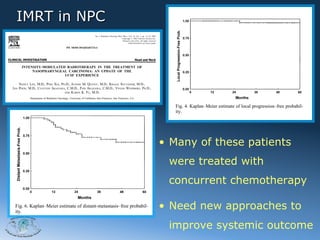

1) Altered fractionation radiotherapy, such as hyperfractionation, can improve survival rates for head and neck cancer compared to standard radiotherapy alone. Hyperfractionation was shown to improve survival by up to 8% according to the MARCH meta-analysis. 2) Intensity-modulated radiation therapy (IMRT) allows for more precise dose delivery to tumor volumes while reducing dose to surrounding healthy tissues, improving outcomes. However, it requires strict quality control protocols to minimize risks from issues like poor delineation or setup errors. 3) Studies show IMRT reduces risks of side effects like xerostomia and blindness compared to other techniques, with one study finding no cases of blindness in patients










































































































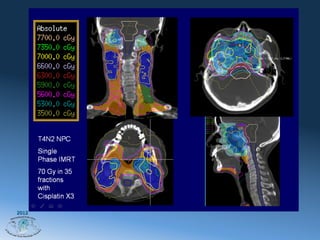
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
