Downloaded 229 times
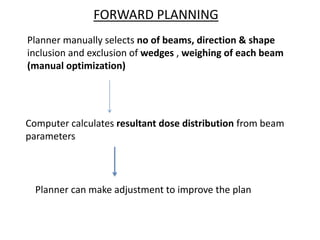
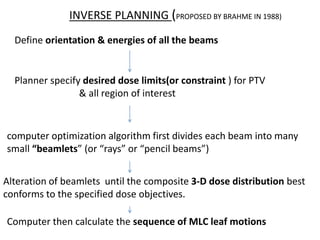
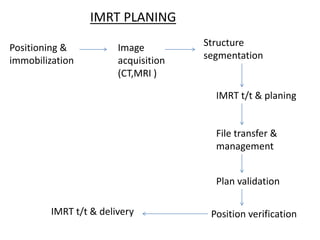

This document provides an overview of Intensity Modulated Radiotherapy (IMRT). It discusses the shift from conventional to conformal radiotherapy using improved imaging and planning techniques. IMRT allows customization of radiation dose distributions through non-uniform beam intensities achieved using dynamic multileaf collimators or compensators. The clinical implementation of IMRT requires treatment planning and delivery systems. IMRT offers advantages over conventional radiotherapy for many cancer types and its use has increased substantially in recent decades.





![Arc therapy [autosaved] [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/arctherapyautosavedautosaved-150423125828-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)










































































