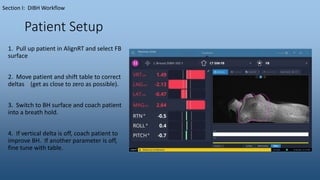
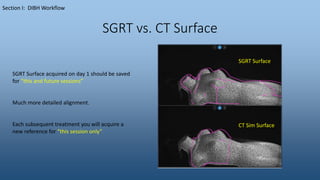
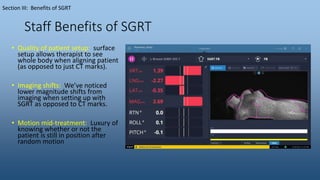
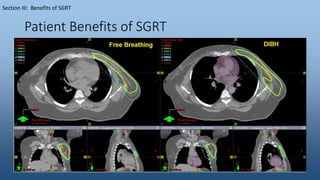
The document outlines the workflow for Deep Inspiration Breath Hold (DIBH) at Cartersville Medical Center, detailing steps from patient simulation to treatment delivery using the AlignRT system. It emphasizes patient education, selection criteria, breath-hold coaching, and the roles of staff during the DIBH process. Benefits of the technique include improved patient setup, reduced tattooing, and effective motion monitoring during treatments.