The document discusses pulse, including its definition, history, components, and how it changes in different conditions. It can be summarized as:
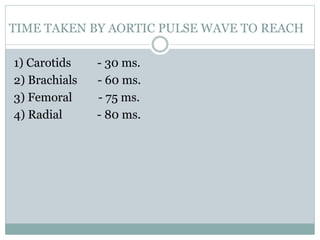
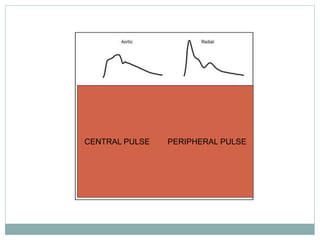
1) Pulse is the palpable wave transmitted from the aorta by the heartbeat and travels faster than blood. It provides information on heart function.
2) Throughout history, physicians have used the pulse to diagnose illnesses, noting characteristics like strength and rhythm. Ancient Chinese medicine especially focused on pulse diagnosis.
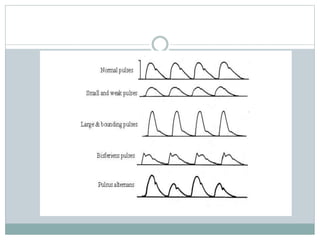
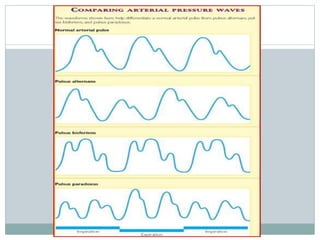
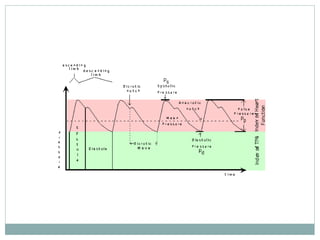
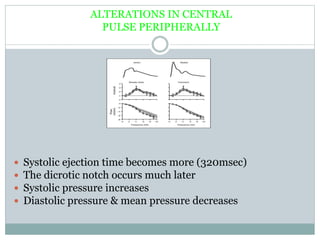
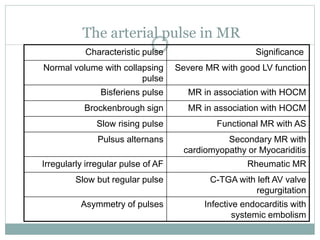
3) The pulse waveform has different components that can be altered by cardiovascular abnormalities like stenosis, regurgitation, or stiff arteries from aging. Abnormal pulses include those that are small, late-peaking, or have other distinctive features.

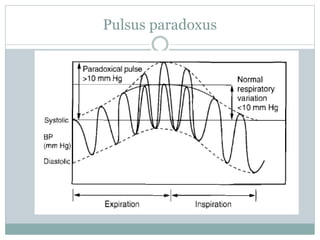
![PULSUS PARADOXUS
LV filling is reduced during inspiration because exaggerated
RV filling causes
1) Leftward shift of IVS reducing LV volume & diastolic compliance
2) Elevated intrapericardial pressure which is transmitted to the LA but
not the extraparenchymal pulmonary veins and hence a decreased
pulmonary vein – LA pressure gradient
3)Inspiratory pooling of blood in the pulmonary bed produces decline in
LA and LV filling.
[Underfilled LV may be operating in the steep ascending limb of Starling
curve so that any inspiratory reduction of LV filling results in marked
depression of the LV stroke volume and the systolic pressure].](https://image.slidesharecdn.com/pulse-copy-240208063926-e8599406/85/PULSE-Copy-ppt-51-320.jpg)